A New Vision for Women's Health Research: Transformative Change at the National Institutes of Health (2025)
Chapter: 7 Overview of Selected Women's Health Conditions
7
Overview of Selected Women’s Health Conditions
A wide range of conditions are specific to females,1 more prevalent among women, or affect women differently than men (see Table 7-1). Moreover, as a result of insufficient research and measurement, it remains unclear the full extent of conditions that uniquely affect women. While it was not possible for the committee to review every women’s health condition in depth, it presents a framework in this chapter for quantifying and categorizing health conditions that affect women’s morbidity, mortality, and quality of life in different ways and selects exemplar conditions to illustrate pressing needs for further research investment in women’s health scientific investigation. Together, the examples across the life course highlighted in this chapter represent those that are present in women and men but progress differently in and cause greater disability in women (e.g., mood disorders) or cause more premature mortality in women compared to men (e.g., cardiometabolic diseases, autoimmune disease, and Alzheimer’s disease [AD]); are female specific and leading causes of death (e.g., gynecological cancers); and are female specific and a leading cause of reduced quality of life and disability (e.g., endometriosis, fibroids, and perinatal and menopause-related depression). Because pregnancy influences the trajectory of cardiometabolic and cognitive disease later in life, the chapter also summarizes its effects across the life course.
___________________
1 The terms “female” and “woman” are used differently according to context and perspective, which may cause confusion (see Chapter 1). In this chapter, the committee uses “female” when discussing specific sex traits related to a specific condition and “woman” when discussing the population more generally (the latter includes all people who identify as a woman or girl, solely or in addition to other gender identities and regardless of biological sex traits).
Two recent National Academies of Sciences, Engineering, and Medicine (National Academies) reports comprehensively reviewed and identified research gaps for two pressing women’s health topics: autoimmune disease and chronic conditions (see Box 7-1 for a summary of the conditions). The findings of those reports corroborate the research needs this committee identified; it relied upon and attempted not to duplicate the effort of these reports. Boxes 7-2 and 7-3 provide a summary of key recommendations to address research gaps from those reports.
BOX 7-1
Women’s Health Conditions Reviewed in Enhancing National Institutes of Health Research on Autoimmune Disease and Advancing Research on Chronic Conditions in Women
Conditions reviewed in Enhancing NIH Research on Autoimmune Disease (2022)
- Sjögren’s disease
- Systemic lupus erythematosus
- Antiphospholipid syndrome
- Rheumatoid arthritis
- Psoriasis
- Inflammatory bowel disease
- Celiac disease
- Primary biliary cholangitis
- Multiple sclerosis
- Type 1 diabetes
- Autoimmune thyroid diseases
Conditions reviewed in Advancing Research on Chronic Conditions in Women (2024)
- Endometriosis/dysmenorrhea/chronic pelvic pain
- Uterine fibroids
- Infertility
- Vulvodynia
- Pelvic floor disorders (including urinary incontinence and pelvic organ prolapse)
- Menopausal symptoms (including exogenous hormone use)
- Systemic lupus erythematosus
- Multiple sclerosis (also affects the neurocognitive system)
- Osteoporosis
- Sarcopenia
- Alzheimer’s disease
- Migraine/headache
- Chronic pain
- Fibromyalgia
- Myalgic encephalomyelitis/chronic fatigue syndrome
- Cardiovascular disease
- Stroke
- Metabolic conditions (Type 2 diabetes, metabolic syndrome)
- Depression
- Substance use disorder
- Human immunodeficiency virus
SOURCES: NASEM, 2022, 2024b.
NOTE: These are a combination of conditions that are female specific, are more common in women, or impact women differently.
BOX 7-2
Enhancing National Institutes of Health Research on Autoimmune Disease: Summary of Recommended Research Priorities
This report identified several crosscutting research needs for autoimmune disease and recommended research to address gaps in knowledge, including to
- Dissect heterogeneity across and within autoimmune diseases to decipher common and disease-specific pathogenic mechanisms.
- Study rare autoimmune diseases and develop supporting animal models.
- Define autoantibodies and other biomarkers that can diagnose and predict the initiation and progression of autoimmune diseases.
- Determine the biologic functions of genetic variants and gene–environment interactions within and across autoimmune diseases using novel, cutting-edge technologies.
- Examine the role of environmental exposures and social determinants of health in autoimmune diseases across the life-span.
- Determine the impact of coexisting morbidities, including co-occurring autoimmune diseases and complications of autoimmune diseases, across the life-span, and develop and evaluate interventions to improve patient outcomes.
- Foster research to advance health equity for all autoimmune disease patients.
SOURCE: NASEM, 2022.
BOX 7-3
Advancing Research on Chronic Conditions in Women: Summarized Research Agenda
The report identified key research gaps that the National Institutes of Health and other relevant agencies that fund research should support to advance the understanding of chronic conditions in women. The following areas of research were recommended to help fill those research gaps.
Recommendation 1: Impact—improve estimates and support national surveillance and population-based studies; expand data collection activities to include female-specific and gynecologic and female-predominant conditions not currently included.
Recommendation 2: Biology and Pathophysiology—understand how gonadal hormones and sex chromosome genes interact to cause sex differences, role of inflammation and immune system, and genetic heterogeneity of conditions (e.g., endometriosis); improve animal and preclinical models.
Recommendation 3: Female-Specific Risk Factors—the specific role of reproductive milestones across the life course (e.g., menarche, pregnancy, perimenopause, menopause, and postmenopause) and address symptoms.
Recommendations 4–6: Disparities and Life Experiences—interaction of multiple social identities with structural and social determinants of health; role of traumatic experiences; role of lifestyle behaviors.
Recommendation 7: Diagnosis and Treatment—improve early and accurate detection and diagnosis of chronic conditions; develop sex- and gender-specific tools; establish better diagnostic tools of conditions that share similar symptoms (e.g., chronic pain, fibromyalgia).
Recommendation 8: Multiple Chronic Conditions—understand biological mechanisms, diagnosis, and treatment and care for women with multiple chronic conditions; develop research approaches to appropriately study and include women with multiple chronic conditions.
Recommendation 9 & 10: Inequities and Women-Centered Research—develop methods for assessing structural determinants of health such as sexism and ageism; recruit women from different backgrounds and use novel techniques for engaging women; account for sex and gender in studies.
SOURCE: NASEM, 2024b.
A FRAMEWORK FOR QUANTIFYING DISEASE BURDEN TO ILLUSTRATE WHR GAPS
This section illustrates the annual burden of disease experienced by women in the United States in terms of years of life lost (YLLs), years lived with disability (YLDs), and disability-adjusted life years (DALYs). Further, it demonstrates through simplified examples how such analyses can help in setting priorities for women’s health research (WHR) by identifying imbalances in health research investments. The committee used this analytic approach to frame the discussion of key exemplar conditions affecting women’s health later in this chapter.
The Value of Research Investment and Metrics for Quantifying Disease Burden
The burden of different health conditions and the opportunities for research to alleviate it (i.e., the expected health return on research investment) are important factors in decisions about allocating a limited pool of funding. Both are difficult to quantify and involve substantial uncertainty; in particular, the latter requires assumptions about potential advancements and breakthroughs. This section describes available metrics to quantify disease burden and explores their application to funding allocation decisions. The committee assumes that investments in women’s health would have at least as much potential for health returns as investments in other areas, which is conservative given the historical underinvestment in WHR described in Chapters 2 and 4. The analysis therefore focuses on quantifying the burden of disease that could be addressed by WHR. In practice, such analyses would ideally consider both of these metrics and other factors, including expected research returns, explicit investment in historically neglected areas, and the minimum threshold needed to ensure progress across a range of areas.
A key challenge for quantifying the burden of disease and comparing the health effects of different conditions is determining comparable outcomes across disease areas. For example, health effects can be measured in terms of people affected using metrics such as incidence (the number of new cases per unit of time, often annually) and prevalence (the number of individuals affected in some time period). Other metrics, such as annual deaths, also reflect disease severity. In comparing diseases, qualitative differences in burden across health problems present critical challenges, such as how to compare the societal health effect of endometriosis, a condition affecting roughly 11 percent of reproductive-age women—approximately 1 in 26 U.S. women—that can cause severe abdominal pain; persistent or recurring genital pain before, during, or after intercourse (dyspareunia); and
infertility, to that of gynecological cancers, which affect approximately 1 in 168 U.S. women but more frequently cause mortality (Buck Louis et al., 2011; Ellis et al., 2022; IHME, n.d.-a; Stewart et al., 2013). A similar challenge is how to compare the effect of a chronic illness, such as asthma, to that of a brief but severe episode of acute illness, such as influenza or COVID-19.
The committee drew on the validated approach of aggregated health metrics, which include both DALYs and related measures, such as quality-adjusted life years. These standardized methods are widely used both nationally and internationally and aggregate nonfatal and fatal health effects into comparable measures (Augustovski et al., 2018; NCCID, 2015; Sassi, 2006). Furthermore, they integrate the type and duration of health effects to quantify burden in a way that can be easily compared across disease areas. Although these measures have limitations, discussed later, such analyses can nevertheless provide insights into comparisons among all women’s health conditions.
Understanding DALYs
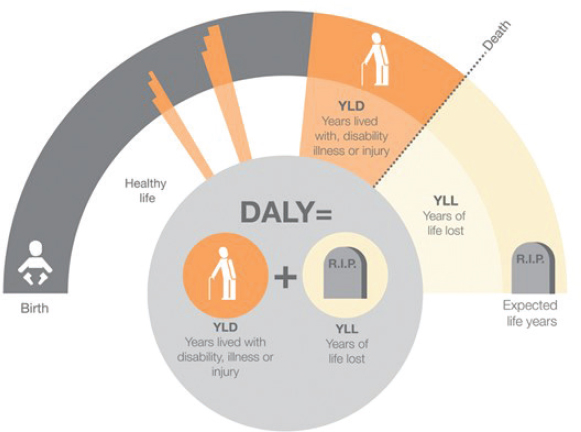
In this chapter, burden of disease is quantified in terms of DALYs, which measure the loss of health resulting from disease or injury, where a year lived in perfect health is denoted as 0 and a year of life lost is denoted as 1. In general, health interventions seek to avert or reduce DALYs. Because health conditions may cause impaired quality of life or loss of life, DALYs are the sum of YLLs and YLDs (Salomon et al., 2012). Figure 7-1 displays this breakdown, with YLDs, marked in orange, accruing both as a result of temporary and chronic conditions and YLLs, marked in beige, showing years of life lost compared to a full healthy life expectancy.
To calculate YLLs, researchers compare an estimate of the average age at death for a particular condition to an estimate of an average full healthy life expectancy. To calculate YLDs, researchers use weights that convert the health burden of different conditions into a number of effective years lost. Usually, standardized DALY weights come from the Global Burden of Disease (GBD) study that presented an international sample of individuals with two descriptions of health states and asked which scenario described a healthier individual (Salomon et al., 2012, 2015). Using another series of questions, these ratings were anchored onto the 0–1 scale described. Given the extremely high correlations across nations,2 researchers designed only one scale of DALY weights, which are regularly updated, calculated in a standard way across conditions, and applied broadly. The weights are publicly available (IHME, n.d.-c; Salomon et al., 2012).
___________________
2 Nations included Indonesia, Peru, Bangladesh, Tanzania, and the United States in 2009–2010, and Hungary, Italy, the Netherlands, and Sweden were added in 2013 GBD analysis (Salomon et al., 2015).
SOURCE: U.K. Health Security Agency, 2015; licensed by Open Government Licence v3.0 (https://www.nationalarchives.gov.uk/doc/open-government-licence/version/3/).
Analyses
This section provides descriptive statistics for the burden of female diseases in estimates from the GBD study, characterizing the burden’s distribution across conditions and comparing it to the male burden. Second, this section uses stylized benchmarking analyses to explore how decision makers may use data that measure the burden of illness in a standardized to inform funding allocation and priority setting decisions in WHR.
Descriptive Statistics
Data
The GBD study regularly provides publicly available and comprehensive estimates of the frequency and burden of all health conditions in the United States by sex. The concept of DALYs is organized into a hierarchical structure with multiple levels to provide a comprehensive view of health loss (see Box 7-4). The committee extracted annual prevalence, incidence, DALYs, YLLs, and YLDs across all available disease areas by sex from GBD 2021 U.S. estimates, the most recent year available, for Level 3 causes, the most granular comprehensive level in the GBD database (IHME, n.d.a). For outcomes of particular women’s health interest, annual incidence and prevalence, the committee benchmarked estimates against external, independent estimates from the peer-reviewed literature, generally finding equivalence, with limitations as noted. The committee excluded COVID-19
BOX 7-4
Disability-Adjusted Life Year Categories
The DALY hierarchical framework has three or four levels, depending on the level of analysis:
Level 1 is the highest level of aggregation and includes noncommunicable diseases; injuries; and a group of infectious diseases, maternal and neonatal disorders, and nutritional deficiencies. This level provides a broad overview of the major types of health issues affecting populations.
Level 2 breaks down the Level 1 categories into more specific risk categories: 22 disease and injury aggregate categories, such as respiratory infections and tuberculosis, cardiovascular diseases, and transport injuries.
Level 3 further refines the risk categories into more specific causes, such as tuberculosis, stroke, and road injuries. In some cases, Level 3 causes are the most detailed classification, while for others, a more detailed category is specified at Level 4.
Level 4 is not consistently defined across conditions, and its use varies depending on the study and level of detail required.
SOURCES: GBD 2021 Diseases and Injuries Collaborators, 2024; IHME, n.d.-b.
from the analysis given its anomalous burden in 2021; burden estimates were otherwise comparable to 2019.
Methods
For reporting and display purposes, the committee aggregated 175 Level 3 conditions into 17 categories, adjusting standardized Level 2 categories to highlight outcomes of interest, such as separating out female-specific cancers. Outcomes are presented by sex, condition, and type in terms of DALYs, YLLs, and YLDs.
Burden of Female Disease
Figure 7-2 summarizes estimated 2021 DALYs by disease category, sex (top panel), and type (bottom panel). Overall, men have a higher number of DALYs than women (who were 49 percent), but women experienced a disproportionate share of disability (55 percent of YLDs). For both, mental health and substance use disorders were the most common DALY categories,

NOTES: The top panel displays DALYs by sex. The bottom panel displays only female-specific DALYs, decomposed into years of life lost (YLLs) and years lived with disability (YLDs).
followed by cardiovascular disease (CVD) and cancer, with men experiencing a majority of DALYs in these conditions. By contrast, among conditions experienced by both men and women, women had a majority of DALYs related to musculoskeletal, chronic respiratory, and neurological conditions.
The bottom panel of Figure 7-2 further breaks down contributions of disability and mortality to the female DALY burden. The dark blue portion of each bar shows the YLLs attributable to each condition. The light blue portion shows DALYs resulting from time spent with disability, such as loss of quality of life through physical or mental health limitations or discomfort. CVD and cancers are the main drivers of YLLs among
women. In contrast, for mental health, substance use, and musculoskeletal disorders, DALYs from mental health conditions are attributable primarily to disability. The former may be, in part, an artifact of GBD coding—several mental health conditions, such as depression leading to suicide and schizophrenia, are also associated with premature mortality (Schoenbaum et al., 2017; Vigo et al., 2022). Some women-specific health conditions, such as female-specific cancers, gynecological problems, and female sexually transmitted infections, constitute a smaller total DALY burden compared to other categories, though female-specific cancers are the fourth-leading cause of premature mortality among women through YLLs. The next section discusses the challenge of connecting the burden of female disease and disability to WHR.
Benchmarking
While these descriptive results characterize the overall burden of disease in women, further analysis would be required to inform funding allocation with disease burden. The following presents two stylized examples of how burden data could inform resource allocation.
Cancer funding is considered as a simplified example of within–National Institutes of Health (NIH) Institute and Center (IC) prioritization; in this case, comparing spending on female-specific and non-female-specific cancers. Approaches to delineating the total burden of disease that research on women-specific diseases and those that affect women disproportionately or differently might address are then explored.
- Cancer spending This is a discrete, well-defined case study that allows comparing investments in female-specific or predominant disease subtypes, including breast, uterine, cervical, and uterine/endometrial, to cancers affecting both men and women. National Cancer Institute (NCI) data were extracted on estimated 2021 spending across 17 cancer types (NCI, 2024e). For each type, spending was divided by total 2019 burden measures (e.g., DALYs, YLLs, YLDs), summed over both sexes, to understand how research investment compared each type’s health burden. Although this exercise is simplified by considering only 1 year of data and crudely comparing female-specific to non-female-specific cancers, this approach can highlight areas of underinvestment relative to disease effects.
- WHR portfolio Next, a more challenging question is considered—the fraction of the total U.S. disease burden falling under the purview of WHR, defined as encompassing conditions that are female specific, are disproportionately female, or affect women
- differently. Most people would not consider research on any disease affecting women to be “WHR,” since that would encompass nearly all modern clinical research, be so overly broad as to obscure the gaps and barriers discussed in this report, and overlook the value of research that studies two sexes. Nevertheless, as this report elucidates, adequately addressing women’s health issues requires understanding sex differences in disease pathways and presentation. Such research is critical for women’s health and well-being, including in domains such as CVD, for which women experience 43 percent of the overall DALY burden.
To provide a simplified schematic that addresses this balance, the committee divided the 175 level 3 GBD categories by those disproportionately occurring in women (more than 67 percent of DALYs); those more common in women (51–67 percent of DALYs); and other conditions (50 percent or fewer DALYs but often occurring differently in women). Next, the committee estimated the proportion of WHR-related DALYs, attributing 100 percent of female DALYs in the first category to women’s health, 50 percent in the second, and 33 percent in the third. This was intended to include contributions of both domains that traditionally fall entirely under the purview of WHR, such as gynecological conditions, and conservatively estimate the need for research powered to detect or focused specifically on sex differences. DALYs were reported by condition, category, and percentage of overall disease burden falling in this category.
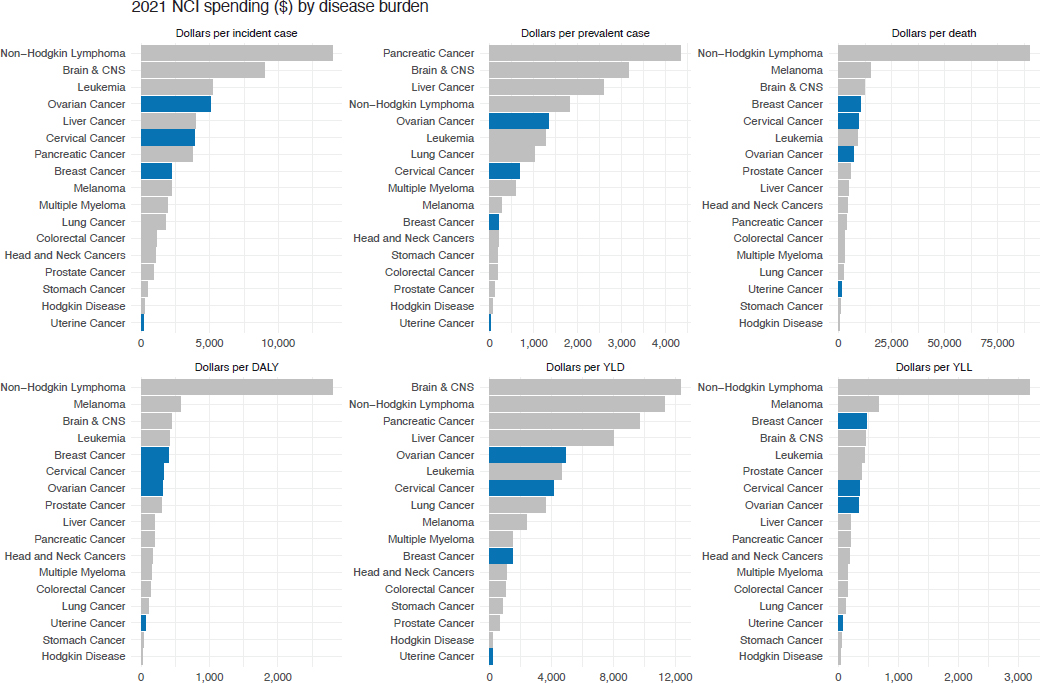
Cancer spending
Figure 7-3 summarizes spending per unit of disease burden across cancer types, summarizing the ratio of fiscal year (FY) 2021 NCI reported spending to 2019 cancer incidence, prevalence, deaths, DALYs, YLLs, and YLDs in males and females. In each case, some female-specific cancers (blue bars) receive less NIH funding than many other cancers. In particular, uterine cancer ($57 per DALY) receives markedly lower funding per DALY compared to conditions such as non-Hodgkin’s lymphoma ($2,794), brain cancer ($444), and pancreatic cancer ($190).
WHR portfolio
Figure 7-4 presents estimates related to a potential WHR portfolio. It highlights important contributions of both female-dominant and specific conditions, such as breast and gynecological cancers and gynecological and maternal disorders, and other conditions (e.g., musculoskeletal, mental health, and substance use disorders) relevant to women’s health.
Overall, this classification encompasses 34 percent of all female DALYs and 16 percent of U.S. DALYs across both men and women. This framework
NOTE: Blue bars indicate female-specific cancers.
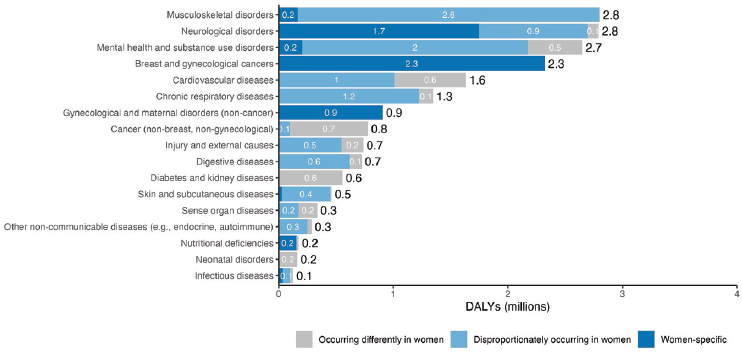
NOTE: These include all female DALYs for female-specific conditions (more than 67 percent of DALY disease burden in women) and a fraction of female DALYs for conditions experienced disproportionately in women (50 percent) or differently in women (33 percent).
is simplified and likely conservative: DALY estimates may be underestimates of the true prevalence of women’s disease burden due to underdiagnosis (see Box 7-5), and as noted, this analysis does not account for lack of investment in basic science related to women’s health (see Chapter 5), which would likely increase relative returns on investment. This rough estimate nevertheless provides a striking benchmark in comparison to the committee’s funding analysis in Chapter 4—for NIH funding on WHR (which averaged 8.8 percent from FY 2013 to FY 2023) to reach this 16.5 percent burden estimate, it would need to increase by nearly twofold (87.5 percent). These burden estimates guide the discussion of conditions in this chapter.
Rare Diseases
One concern is that metrics focusing on population prevalence overlook rare diseases; funding research in proportion to DALYs would risk stunting progress toward preventing and treating rare illnesses.3 In practice, there is a strong societal preference for investment in serious disabling conditions, even if they affect only a small number of people. Furthermore, making therapeutic progress for any condition requires a minimum threshold of investment, which may require funding rare conditions disproportionately to burden.
___________________
3 According to the Orphan Drug Act, a disease or condition is considered rare if it affects fewer than 200,000 Americans (Public Law 97–414). [This footnote was changed after release of the report to clarify the source of the definition.]
DALYs per affected individual may also be considered to illustrate the concentration of disease burden. Nevertheless, tradeoffs remain challenging: how is a rare, severe neurological condition, such as Rett syndrome, which affects only one in 10,000 female individuals, weighted against a much more common but less debilitating condition, such as endometriosis or osteoarthritis?
A Framework for Selecting Exemplar Conditions Illustrating WHR Gaps
Several limitations to these analyses—and the use of DALYs or aggregated metrics more broadly—may merit consideration or further study when using disease burden analysis to identify research gaps and support funding decisions (see Box 7-5). Although DALYs are an imperfect metric, they
BOX 7-5
Limitations of Disability-Adjusted Life Years and Future Directions for Health Metrics
DALYs and other aggregated health metrics can only provide insight related to the burden of disease for specific conditions. This approach is less useful for informing less-targeted basic science research or research focused on health-promotion, such as supporting contraceptive use.
There are also several limitations specific to the GBD study calculation of DALY weights.
- Weights were calculated by soliciting paired comparisons about the “health” of individuals experiencing various conditions. Some conditions, such as infertility, may substantially affect quality of life but have a low disability weight due to perceptions that the impact does not fall into the category of “unhealthy.”
- GBD weights are being updated, particularly to account for women’s health conditions. For example, new weights for dyspareunia and chronic conditions will be in a forthcoming update.
- In some cases, GBD burden estimates differ from those in other sources. For example, GBD reports a much lower prevalence of endometriosis than other estimates. This may arise because GBD prevalence estimates are differentially affected by diagnosis. For example, estimates of premenstrual disorder include self-reported survey responses, while endometriosis requires surgical diagnosis.
Additional research to contextualize DALYs to account for differential circumstances in which disability is experienced, such as social support and economic resources, would be valuable.
remain a widely applied measure that allow comparisons across diseases and sequelae. Therefore, despite these limitations, the committee found this to be a useful framework for identifying exemplar conditions to illustrate WHR needs and create a matrix of women’s health conditions (see Table 7-1). Some conditions could fit into two categories, but for this overview, conditions are discussed in the DALY category based on the committee’s analysis.
EXEMPLAR WOMEN’S HEALTH CONDITIONS
In this section, the committee provides a brief overview of some of the research gaps that fall into the categories identified in the matrix in the DALYs section (see Table 7-1).
FEMALE-SPECIFIC CONDITIONS WITH INCREASED DALYS RESULTING FROM DISABLING CONDITIONS
The 2024 National Academies report Advancing Research on Chronic Conditions in Women reviewed several female-specific conditions that increase DALYs as a result of disability and affect a significant proportion of women (NASEM, 2024b). This section highlights and summarizes several of these conditions, including uterine fibroids (leiomyomas), endometriosis, pelvic floor disorders, and female-specific mental health conditions (see NASEM, 2024b for an in-depth overview of these conditions).
Gynecological Conditions
Fibroids
Fibroids are the most common solid tumor of the pelvis and the leading cause of hysterectomy in the United States (Bulun, 2016; Marsh et al., 2024). While benign, they can lead to significant symptoms, including irregular and excessive uterine bleeding, lower abdominal pressure, dyspareunia, pelvic pain, recurrent pregnancy loss (RPL), infertility, and adjacent organ compression (Bulun, 2016; Marsh et al., 2024; NASEM, 2024b). Fibroids are more common in African American and Black females (Eltoukhi et al., 2014), who are also more likely to develop uterine fibroids at an earlier age, have larger-sized and greater number of fibroids, and experience more severe symptoms (Marsh et al., 2024). Despite their high prevalence, little is known about their pathophysiology. While researchers have studied estrogen as a mitogen for myoma growth, little research has been done to understand the role of other hormonal and non-hormonal factors in fibroid development and why they are more prevalent in Black females (Bulun, 2016; Cetin et al., 2020; NASEM, 2024c; Reis et al., 2016; Sefah et al., 2022). Given the high prevalence and morbidity, additional research
TABLE 7-1 Matrix of Women’s Health Conditions
| Affect only females | Affect only females | Affect only females | Differentially or disproportionately affect women | Differentially or disproportionately affect women | Differentially or disproportionately affect women |
| DALYs resulting from disabling conditions | DALYs resulting from early mortality | DALYs resulting from disabling conditions AND early mortality | DALYs resulting from disabling conditions | DALYs resulting from early mortality in women, and/or mortality in women versus men | DALYs resulting from disabling conditions AND early mortality in women, and/or early mortality in women versus men |
| Large population effect on females | |||||
|
|
|
|
|
|
NOTES: This table does not cover all conditions that affect only females or disproportionally or differentially affect women; it is a selection of conditions based on the committee’s DALY analysis. For example, additional important female-specific conditions include vulvar and vaginal cancers and vulvodynia. DALY = disability-adjusted life year; * Breast cancer does affect men, but less than 1 percent of all U.S. breast cancer diagnoses are in men.
is needed across the entire translational spectrum to better understand the pathophysiology so that novel targeted medical and surgical treatments can be developed and disseminated (NASEM, 2024b).
Endometriosis
Despite endometriosis being one of the most common causes of infertility and chronic pelvic pain, its cause, risk factors, and true incidence remain uncertain (NASEM, 2024b; Young, 2024). It has no nonsurgical approach to diagnosis, and surgical treatments requiring hysterectomy and hormonal medical treatments are incompatible with fertility and fecundity (Young, 2024). It is also a risk factor for development of ovarian cancer and other chronic pain conditions, including irritable bowel syndrome (Barnard et al., 2024; Nabi et al., 2022). A population-based study found that those who developed endometriosis were 4.2 times more likely to develop ovarian cancer compared to those without endometriosis (Barnard et al., 2024). Additional research is needed to understand the pathophysiology and develop fertility-sparing approaches to treat this debilitating condition.
Pelvic Floor Disorders
Pelvic floor disorders, which are also common and significantly affect quality of life, lead to pelvic organ prolapse, urinary and fecal incontinence, recurrent urinary tract infections, bladder pain syndrome, and myofascial pelvic pain. Pelvic organ prolapse specifically occurs in up to 50 percent of female patients, but there are significant knowledge gaps in the basic science understanding of normal and abnormal pelvic floor function and the structural aspects of pelvic floor support (Aboseif and Liu, 2022; Swenson, 2024). A better understanding of pelvic floor function and its hormonal, structural, and functional determinants will enable more effective interventions. These are sorely needed given the high surgical treatment failure rate, impairing female quality of life (Swenson, 2024).
Polycystic Ovary Syndrome (PCOS)
PCOS is the most common endocrine disease in female patients and a leading cause of female impaired fecundity (Akre et al., 2022). It is a complex hormonal, metabolic, and reproductive disorder affecting multiple organ systems and afflicting approximately 4–18 percent of reproductive-age females (Bozdag et al., 2016; Dennett and Simon, 2015). Research has yet to fully elucidate the etiology, although in the majority of patients, it appears to be linked to some combination of polycystic ovarian morphology, hyperandrogenism, and ovulatory dysfunction. Many people are
unaware they have it, as it is often characterized by myriad heterogenous signs and symptoms. The Rotterdam diagnostic criteria are the most accepted, requiring two of the following three features: hyperandrogenism, oligo- or anovulation causing missed or irregular periods, or polycystic ovaries (Christ and Cedars, 2023). The hyperandrogenic state is proposed to contribute to insulin resistance and hyperglycemia and ultimately adiposity, or excessive body fat accumulation. PCOS can lead to significant medical conditions, including CVD, Type 2 diabetes, impaired fecundity, fatty liver disease, endometrial hyperplasia, and endometrial cancer, some of which may develop as a function of higher levels of body fat. It has no cure and no Food and Drug Administration (FDA)–approved therapies (Allen et al., 2022; Dennett and Simon, 2015; NASEM, 2024c).
Additional research is needed to better delineate the underlying cause; understand the complex interplay of genetic, epigenetic, and environmental factors associated with PCOS; identify curative therapies; assess long-term cardiovascular, metabolic, and cognitive decline risks; and identify mitigation strategies to prevent comorbid conditions (Che et al., 2023; Christ and Cedars, 2023). Recent research has also highlighted the need for further investigations on PCOS and its relationship to brain health during midlife (Huddleston et al., 2024). Despite its prevalence among females and substantial research gaps, PCOS also ranks near the bottom among NIH-funded conditions, according to the committee’s funding analysis (see Chapter 4).
Additional gynecological conditions that take a significant toll on the lives of women and lead to disability are discussed in the 2024 report, including vulvodynia (NASEM, 2024b). The committee heard from many brave individuals who shared their experiences with gynecological conditions during the committee’s information-gathering stage; see Box 7-6 for some of their experiences.
Funding Shortfall
A significant challenge to advancing research on these female-specific conditions is that noncancer gynecological conditions lack an NIH funding home among the current ICs. Figure 7-5 illustrates this contrast—even though more females are affected by endometriosis and PCOS than breast cancer, there is a paucity of funding for these conditions relative to breast cancer. Without a dedicated funding stream and NIH study sections that include the proper scientific expertise to review grants submitted on these conditions, there is a missed opportunity to advance scientific discoveries and treatments that will significantly improve quality of life and productivity for a significant proportion of the female population. It is critical to increase funding for these conditions to be on par with female-specific cancers.
BOX 7-6
In Their Own Words: Excerpts from Patients and Patient Advocates on Gynecologic Conditions During Public Comments at Committee Meetings
Polycystic Ovary Syndrome (PCOS)
- There isn’t enough funding for research across women’s health, but PCOS is an interesting case where it’s a really prevalent disorder globally impacting 8 to 13 percent of women. Yet PCOS wasn’t even listed in NIH’s Research Condition Diseases Category reporting, the RCDC, until our organization’s advocacy work. And so, this highlights that there are certain aspects of women’s health which haven’t been prioritized even though it impacts so many of us.
- We need to implement policies to ensure equitable funding and focus across diseases affecting women of all backgrounds. PCOS disproportionately impacts women of color and their metabolic health, mental health, et cetera, yet there is very little funding in this area, and very few Black researchers who are getting funded. So, thinking about not only who we are studying but who’s doing the research and care as well.
Pelvic Floor Disorders
- Pelvic floor disorders cause musculoskeletal dysfunction, pain, loss of productivity, decline in self-esteem, relationship difficulties, mental health issues, just to name a few. Frequently, for pelvic floor research, we may see a study done with 30 subjects or a case study done with 1–3 people simply because NIH has not funded or prioritized research in this area. The data are shocking.
- Pelvic floor research is divided throughout NIH, and it has not focused on women’s pelvic health through the life-span. The result is, without research data, the diagnostic criteria is variable. We don’t have well-researched treatment options. Therefore, women cannot get the treatment and the services they need covered by health care.
Fibroids
- The lived experience of women with uterine fibroids is, I believe, a societally dismissed experience in communities worldwide that is steeped in a millennia old stigma that is expected that women will endure immense pain. Today in many countries women are still community outcast during their menstrual cycles.
Endometriosis
- I’m not being alarmist when I say the lives of more than 6 million women nationwide quite literally depends on [more research]. Endometriosis has affected every single aspect of my life. It has ravaged my body beyond repair, destroyed relationships, stripped me of identity.
- At just 27 years old, it forced me to go on medical disability from work for over a year. It forced me to drop out of graduate school, just one class short of earning a master’s degree. And I wish my story of turmoil and loss due to endometriosis were unique, but sadly, it is just one of millions.
- Despite my medical background and knowledge, it still took me over 4 years and 10 specialists ranging from pulmonology to cardiothoracic surgery to gastroenterology to be officially diagnosed with diaphragmatic endometriosis.
Vulvodynia
- Despite how common this condition is, it took years of going from doctor to doctor to get diagnosed. Clinicians told me to drink wine to relax before sex and seemed to incorrectly attribute my pain to something psychological. Meanwhile, I was trying to figure out how to sit and move without hurting. This was one of the most upsetting and isolating periods of my life, trying to find out why I was having this severe and terrifying pain, and why no provider seemed to take it seriously.
- Diagnosis was half the battle; treatment is another. I spent years trying every imaginable treatment and medication. Everything I have tried was off-label since there is no FDA-approved drug for any kind of chronic vulvovaginal pain. There is an effective surgery but it’s only done by a few surgeons in the country and can cost tens of thousands of dollars out of pocket.
- It’s daunting to stare down a lifetime of chronic pain, and it is made so much worse by the fact that most doctors, even OB-GYNs, have not heard of this issue. We need hope that some attention is going to be paid to finding effective treatments for this devastating diagnosis.

SOURCE: Committee’s funding analysis (see Chapter 4).
Mental Health Conditions
Perinatal Depression
Perinatal depression, a major depressive disorder that occurs during pregnancy or in the first 12 months following childbirth, appears in approximately 10–20 percent of pregnancies in the United States and, along with other mental health conditions, is the leading cause of maternal mortality, accounting for 23 percent of maternal deaths (Dagher et al., 2021; Payne and Maguire, 2019; Sayres Van Niel and Payne, 2020; Trost et al., 2022). Specifically, 1 in every 7–10 pregnant people and 1 in every 5–8 postpartum people develop a depressive disorder, which translates to more than a half million cases each year, approximately the same number diagnosed with diabetes (Sayres Van Niel and Payne, 2020). Like diabetes, perinatal depression is a costly and potentially fatal condition, with its annual cost totaling at least $15 billion, or more than $22,600 per mother and infant, yet unlike diabetes, 91–93 percent of those with perinatal depression do not receive effective treatment (Cox et al., 2016), an enormous gap in clinical care.
As discussed in Chapter 5, NIH investment in research to understand the neuroendocrine mechanisms of perinatal depression resulted in
two FDA-approved, highly effective treatments using allopregnanolone, a neuro-receptor modulator. It took over 80 years, however, from compound discovery to translation to treatment, and despite the advances, research funding for allopregnanolone and perinatal stress and depression remained much lower than other chronic conditions, such as breast cancer, afflicting a similarly large segment of the U.S. population (Deligiannidis, 2024; Pinna, 2020; Reddy et al., 2023). This funding trend has persisted (see Chapter 4 for more information), and important barriers to care, including a lack of screening and diagnosis, prevent most women from receiving effective treatment.
Psychotherapy is the first-line treatment for perinatal depression (Cuijpers and Karyotaki, 2021), and 92 percent of pregnant people prefer individual therapy to group treatment or medication (Goodman, 2009). However, only 7 percent of those with perinatal depression receive effective treatment because of systemic barriers to care (Cox et al., 2016), including cost, limited numbers of mental health specialists, geographic distance from specialty clinics, scheduling challenges arising from work-related and childcare demands, and stigma associated with seeking mental health care (Byatt et al., 2012; Dagher et al., 2021; Hellberg et al., 2023).
Moreover, although the new fast-acting, FDA-approved medications reduce depressive symptoms more rapidly and to a greater degree than earlier medications, they are not effective for about one-third of females; can only be used in the postpartum period, even though most cases of perinatal depression begin during pregnancy; have not been tested in lactating women; cannot be used as a prophylactic; and may be difficult to access given the cost and need for specialist prescribers and specialized treatment facilities that can provide inpatient hospitalization in facilities with 1:1 nursing supervision, for example (Meltzer-Brody et al., 2018; Patterson et al., 2024; Reddy et al., 2023). Of all the reproductive-related mood disorders, perinatal depression has received the most funding and has the strongest scientific foundation upon which to build rapid advances in identifying neurobiological mechanisms, objective diagnostics, novel treatments, and prevention, but realizing that potential still requires substantial monetary investment (Deligiannidis, 2024).
Menopause-Related Depression
The transition to menopause, or perimenopause, is characterized by irregular menses, vasomotor symptoms, sleep and sexual disturbances, weight gain, lassitude, cognitive dysfunction, vaginal dryness, urinary symptoms, and mood symptoms (Woods and Mitchell, 2005). The most commonly studied mood symptom is depression, but other common ones
include irritability and anxiety (de Wit et al., 2021; Rössler et al., 2016; Seritan et al., 2010). Depression risk increases up to 14-fold in the 2 years surrounding the menopause transition (Schmidt et al., 2004), implicating ovarian hormone change as a trigger. Prospective longitudinal studies indicate this transition as a period of increased risk for both depressive symptoms and depressive disorders (Schmidt et al., 2004). With approximately 73 million U.S. women over age 45 (Statista, 2023), more than 1 million women reach menopause every year, and up to 70 percent will experience psychogenic symptoms associated with perimenopause and postmenopause (including anger/irritability, anxiety/tension, and depression) (NIA, 2022; Peacock et al., 2023). Depression (and anxiety) reduce health-related quality of life more than any of the other symptoms related to mental health (Wariso et al., 2017; Whiteley et al., 2013), contributing to the $326.2 billion annual cost associated with depression in the United States (Greenberg et al., 2021).
While research has shown that hormonal changes during perimenopause can affect mood, the precise mechanisms by which these fluctuations lead to depression are not fully understood, and studies are needed to elucidate the roles of estrogen, progesterone (PG), and other hormones in mood regulation during this time (Alblooshi et al., 2023; Bromberger and Epperson, 2018). In addition, factors such as stressful life events, social support, and attitudes toward aging and the menopause transition can influence the onset of depression. However, the interplay between these psychosocial factors and biological changes is not well characterized, representing a major research gap (Bromberger and Epperson, 2018). Although hormone therapy is commonly used to treat menopausal symptoms, its effectiveness as a monotherapy and use in combination with other treatments, specifically for menopause-related depression, merits more robust research (Gnanasegar et al., 2024; Maki et al., 2019). Studies on the long-term effects and safety of hormone therapy for mental health are needed as well. Without a clear understanding of the biological mechanisms driving menopause-related depression or well-powered studies to identify efficacious treatments, clinicians lack the evidence base needed to guide patient care.
FEMALE-SPECIFIC CONDITIONS WITH INCREASED DALYS RESULTING FROM EARLY MORTALITY
This section discusses female-specific cancers that are leading causes of early mortality in women and their variable progress based on NIH investment in research funding. Although breast cancer could fit in this category, it is discussed in the increased DALYs resulting from disability and early mortality section.
Uterine Malignancies
Uterine malignancies, including endometrial carcinomas and uterine sarcomas, are the most common and leading cause of gynecologic cancer. Over the past 2 decades, incidence and mortality rates for uterine cancers have risen alarmingly (Clarke et al., 2019; NASEM, 2024c; NCI, n.d.-d; Whetstone et al., 2022). It is estimated there will be 67,880 new cases and 13,250 deaths from uterine malignancies in 2024, representing 3.4 percent of all new cancer cases, with significant race-related survival disparities (NCI, n.d.-d; Siegel et al., 2024). The 5-year relative survival rate is 84 percent for White women and 63 percent for Black women (Whetstone et al., 2022).
The increasing rates of this disease, rising mortality, and alarming race-related disparities in endometrial cancer necessitate identifying and addressing research gaps (Siegel et al., 2024). Specifically, research is needed to understand the relationship between sex hormones, body weight, inflammation, environmental factors, and social determinants of health (SDOH) in disease etiology; develop prevention strategies and better diagnostic tools; and develop novel FDA-approved treatments. Prevention efforts will need to focus on balancing hormones, weight management, and physical activity (Bae-Jump, 2024). The advent of immunotherapy has seen a dramatic improvement in survival rates for individuals diagnosed with advanced disease, but an approach is lacking for identifying women most likely to benefit from these treatments (Tillmanns et al., 2024). Additional research is needed to assess and validate novel biomarkers of molecular classification to identify patients most likely to respond to therapy and elucidate resistance mechanisms for those who fail to respond to chemotherapy, immunotherapy, and the emerging antibody-drug conjugates.
Ovarian Cancer
Ovarian, tubal, and peritoneal cancer, collectively called “ovarian cancer,” is an often lethal gynecologic malignancy, with 19,680 new cases and 12,740 deaths anticipated in 2024 (NCI, n.d.-c). Screening and early detection of ovarian cancer are challenging, and efforts to improve that have been unsuccessful and did not reduce mortality; it is therefore most common for cancer to be in a late stage at diagnosis (Buys et al., 2011; Karlan, 2024; Menon et al., 2021; NASEM, 2024c). While the incidence and mortality rates are declining, successful cures for this lethal disease remain elusive (American Cancer Society, 2024a). The landscape of ovarian cancer treatment shifted dramatically for high-grade serous—the most common type—and endometrioid cancers with the incorporation
of maintenance poly(ADP-ribose) polymerase (PARP) inhibitor therapy. Since the approval of olaparib in 2018, several other PARP inhibitors have been approved to treat epithelial ovarian cancer or undergone evaluation (Coleman et al., 2017, 2019; González-Martín et al., 2019; Moore et al., 2018). Maintenance PARP inhibitor therapy for newly diagnosed ovarian cancer patients improved progression-free survival significantly, with the greatest benefit seen for those with BRCA-mutated cancers, followed by those with cancer that is homologous recombination deficient (Karlan, 2024; NCCN, 2024). Identifying active treatment options for patients with non-homologous-recombination-deficient epithelial ovarian cancers and primary platinum resistant disease is an important research need (Karlan, 2024).
Specific critical gaps in ovarian cancer include screening, understanding mechanisms of resistance to platinum-based chemotherapy and PARP inhibitor therapy, identification of treatment options for patients who progress on PARP inhibitor therapy, biomarkers to better identify homologous recombination deficiency, and identification of novel therapies beyond PARP inhibitors and emerging antibody-drug conjugates. Gaps to address for rare ovarian cancers, such as nonserous epithelial cancer, germ cell tumors, and stromal tumors, which tend to occur in younger women (Al Harbi et al., 2021; Berek et al., 2021), include developing representative animal models to understand pathophysiology and guide innovative therapies.
Cervical, Vulvar, and Vaginal Cancers
Most cervical, vulvar, and vaginal cancers are caused by human papillomavirus (HPV). Other risk factors include immune system suppression, long-term use of oral contraceptives, cigarette smoking, and prenatal exposure to diethylstilbestrol. In 2024, there will be an estimated 13,820 new cases of cervical cancer and 6,900 cases of vulvar cancer, accounting for 4,360 and 1,630 deaths, respectively (Siegel et al., 2024). The NCI “Last Mile” Initiative Self-Collection for HPV Testing to Improve Cervical Cancer Prevention Trial is assessing HPV self-collection for testing to prevent cervical cancer (NCI, n.d.-a). While this study will help address screening barriers, gaps remain regarding the multifactorial issues that negatively affect follow-up assessment of patients with abnormal screening results, access to care, and improving cure rates (NCI, n.d.-a; Rimel et al., 2022). Additional gaps in research remain regarding the role of induction immunotherapy, radiotherapy sequencing, optimal radiation therapy techniques, understanding mechanisms of resistance to immunotherapy and other novel therapies, and treatment of non-HPV-associated aggressive cervical, vulvar, and vaginal cancers.
Benefits of Funding Research on Female-Specific Cancers
There have been repeated calls to increase funding for research in gynecological cancers. As noted, uterine cancer ranks particularly low in NCI funding across a range of metrics that benchmark funding against population health impact. In 2021, for example, it ranked last in spending per YLDs and third to last in spending per YLLs. Cervical and ovarian cancer also rank below several cancers—including prostate, brain/central nervous system, and leukemia—in spending per YLL. Furthermore, although gynecologic cancers are rarer than, for example, breast, lung, prostate, and colorectal cancer and contribute to a smaller number of total DALYs and YLLs, prognosis remains poor, as quantified in recent gynecological oncology studies that measured YLL per incident case (described as “funding to lethality scores”) (Guevara et al., 2023; Spencer et al., 2019). Greater investment in treatment for gynecological cancers may therefore substantially reduce dire health consequences experienced by many people with these conditions.
The benefits of funding research for female-specific cancers are illustrated by the congressionally directed Department of Defense Ovarian Cancer Research Program (OCRP), initiated in 1997 to support high-impact, cutting-edge research to address the unmet needs in ovarian cancer (CDMRP, 2024). From 1997 to 2022, it funded 633 awards, and 2023 had 298 applicants for awards, of which 42 were funded. Over the 27 years since the inception of OCRP, ovarian cancer incidence and mortality rates have declined (NCI, n.d.-c), and it is easy to speculate that OCRP’s investment of over $496 million in ovarian cancer research was pivotal. For example, OCRP-funded studies have yielded transformative research tools, preventive tests, biomarkers to direct therapy, and novel treatments in the scientific and clinical arena. This includes several distinct novel ovarian cancer animal models; genetic testing guidelines; genetic risk test kits for RAD51D, PALB2, and BARD1 mutations; algorithms to diagnose precursor serous tubal intraepithelial carcinoma lesions; companion biomarker tests to direct PARP inhibitor therapy; and novel therapies (CDMRP, n.d.).4 In contrast, lack of investment in other gynecologic cancers has coincided with rising incidence and mortality of endometrial cancer and stagnant mortality rates in cervical cancer, with disproportionately worse survival outcomes in Hispanic and non-White women and the greatest burden on Black women (NASEM, 2024c; NCI, n.d.-b,d; Siegel et al., 2024).
___________________
4 One such novel therapy is rucaparib, which received accelerated FDA approval for treating patients with BRCA-mutated recurrent ovarian cancer in 2016 and later for maintenance treatment for select patients with platinum-sensitive disease. FDA has approved it for BRCA-mutated metastatic castration-resistant prostate cancer (FDA, 2016).
FEMALE-SPECIFIC CONDITIONS WITH INCREASED DALYS RESULTING FROM DISABLING CONDITIONS AND EARLY MORTALITY
Breast Cancer5
Breast cancer rates have increased by approximately 0.6 percent per year since the mid-2000s, with a slightly steeper incidence in women younger than age 50. It is the most common cancer in women other than skin cancers. The American Cancer Society estimates that 2024 will have approximately 310,720 new cases of invasive breast cancer and 56,500 new cases of ductal carcinoma in situ, and 42,250 women will die from breast cancer (American Cancer Society, 2024b).
Despite significant gaps in breast cancer research, investment has significantly affected mortality rates, with striking improvements in mortality over past decades that reflect multiple moderate gains from screening and treatment improvements (Jagsi, 2024). Increased NIH funding has led to breakthroughs in early detection methods, such as improved mammography and the development of genetic testing, allowing for earlier diagnosis and intervention, as well as improved medications that reduce breast cancer mortality and recurrence (see Box 7-7). Surgical techniques have evolved from radical mastectomies to more conservative approaches, such as lumpectomies and focused and targeted lymphadenectomy, minimizing the physical and emotional impact while maintaining efficacy (Jagsi, 2024). Radiation therapy has also seen progress with more precise targeting methods, reducing damage to healthy tissue and improving outcomes. Chemotherapy has become more effective with the introduction of targeted therapies and less toxic drug regimens, allowing for more personalized and effective treatment plans (Jagsi, 2024). NIH-funded studies have advanced the understanding of how the immune system interacts with breast cancer, which has contributed to developing immunotherapeutic approaches, including checkpoint inhibitors and vaccine therapies, that are now being explored in clinical trials (Al-Hawary et al., 2023; Morrison et al., 2024; Nordin et al., 2023; Pallerla et al., 2021).
Although these investments have paid off in terms of decreasing morbidity and mortality, the journey to preventing and treating breast cancer is not over. Gaps remain in translating many of these discoveries into practice. For example, the U.S. Preventive Services Task Force has concluded there is insufficient evidence to determine the benefits and harms of screening mammography among women aged 75 and older and of supplemental screening
___________________
5 Although breast cancer does affect men, less than 1 percent of all U.S. breast cancer diagnoses are in men (NCI, 2020).
BOX 7-7
NIH-Funded Breast Cancer Prevention and Treatment Discoveries
- In 1958, chemotherapy drugs were used at the NIH Clinical Center to treat solid tumor cancers (including breast cancer), which is now a standard treatment.
- Breakthroughs in imaging technologies (e.g., 3-D mammography) and new biomarker-based tests have improved early detection and diagnosis, allowing for earlier and more precise intervention.
- Research helped identify breast cancer subtypes based on tumor molecular features, which allows for more targeted treatments, contributing to a 41 percent decrease in death rates from 1990–2019.
- In 2012, an NIH-funded study found that a combination of two drugs can lengthen the lives of postmenopausal women with the most common type of metastatic breast cancer.
- Research that identified and characterized the BRCA gene mutations in breast, ovarian, prostate, and pancreatic cancer, which allows individuals with a family history of these cancers to use genetic test results to inform decision making for screening, prevention, and treatments.
- Research has led to developing new drugs that target specific aspects of breast cancer biology. For example, aromatase inhibitors are a standard treatment for postmenopausal women with hormone receptor–positive breast cancer, and CDK4/6 inhibitors have also improved treatment options for this type of breast cancer.
- NIH research led to the discovery and clinical use of drugs such as trastuzumab (Herceptin) for HER2-positive breast cancer and significantly improved outcomes for patients with this subtype.
SOURCES: Early Breast Cancer Trialists’ Collaborative Group, 2015; Morrison et al., 2024; NIH, 2013, n.d.-a; Santen et al., 2009; Ulm et al., 2019.
with ultrasonography or magnetic resonance imaging in women with dense breasts (USPSTF, 2024). Additionally, although robust evidence shows some women can safely avoid potentially toxic treatments, that does not always translate into practice, and many women pursue unnecessarily aggressive treatments, leading to worsened quality of life, second malignancies after unnecessary radiation, and other side effects, such as cardiac toxicity, cognitive decline, and financial toxicity (Jagsi et al., 2017; NASEM, 2024c). Additional research is needed to prevent and treat metastatic breast cancer
and to elucidate the biological mechanisms driving metastasis, including how cancer cells evade the immune system and survive in distant organs.
Racial and Ethnic Survival Disparities in Breast and Gynecologic Cancers
Significant racial and ethnic survival disparities for individuals diagnosed with breast and gynecologic cancers have been reported since the 1970s (Towner et al., 2022). Despite this knowledge, gaps in care have not been completely addressed, leading to persistent and detrimental survival disparities. Overall, the age-standardized death rate for all cancers is highest for non-Hispanic Black patients compared to all other racial and ethnic groups (Cronin et al., 2022). Survival disparities are most striking for uterine cancer, the only cancer for which mortality rates have increased over the past 4 decades (Siegel et al., 2024). Its increased incidence is most pronounced among those who identify as Black, Asian American, Pacific Islander, and/or Hispanic, with a greater than 2 percent increase since the mid-2000s (Siegel et al., 2024). The most alarming racial survival disparity is between Black and White patients; Black people with uterine cancers have a twofold increased risk of death (Siegel et al., 2024). In 2018, the 3-year survival rates were only 69.1 percent in Black patients compared to 86.5 percent in White patients (NCI, 2024d).
Conversely, since about 2000, death rates for breast and ovarian cancer have decreased, while mortality rates have remained stagnant for cervical cancer patients (Siegel et al., 2024). However, Black people with breast, ovarian, and cervical cancers also have worse outcomes compared to White people for every stage of diagnosis (Siegel et al., 2024). For breast cancer, the 3-year relative survival rates in 2018 were 94.8 versus 88.8 percent for White and Black patients, respectively (NCI, 2024a,b). Similar trends were reported for ovarian cancer in 2018, with 3-year relative survival rates of 61.5 versus 55.5 percent for White and Black patients, respectively (NCI, 2024f). For cervical cancer, Black, Hispanic, and American Indian/Alaska Native patients still have the highest incidence and mortality rates compared to White and non-Hispanic patients (AARC, 2024; NCI, n.d.-b; Siegel et al., 2024). Furthermore, screening tests are less likely to be obtained for Hispanic patients compared to White and Black patients (AARC, 2024). The 3-year relative survival rates for cervical cancer are 74.4 versus 64.8 percent for White and Black patients, respectively (NCI, 2024c).
Additionally, Black and Hispanic women with breast, ovarian, cervical, and endometrial cancer are less likely to receive care that adheres to current guidelines (AARC, 2024; Hinchcliff et al., 2019; Siegel et al., 2024; Zhang et al., 2020a). Marginalized patient populations are also less likely to be represented in clinical trials (Scalici et al., 2015); including them is imperative to ensure improved understanding of racial and ethnic differences in
tumor biology, biomarkers, response to therapy, and survival outcomes. Cancer survivors who identify as Black and Hispanic/Latina have poorer quality of life and mental health compared to White or other racial and ethnic groups, respectively (AARC, 2024).
Research has improved understanding of the underlying molecular biology of disease. However, significant gaps remain. More research is needed to understand the underlying etiology of racial and ethnic survival disparities and intersections with SDOH. Dedicated funding to address cancer disparities for female-specific cancers are critical to mitigate racial and ethnic survival disparities and ensure equitable care for all patients.
Maternal Disorders/Pregnancy-Related Complications
Each year, there are 5.5–6.5 million pregnancies in the United States. Despite the incredibly common nature of pregnancy, its understanding along the translational science spectrum from basic science to population health outcomes and policy impact remains poor. In fact, even the precise number of pregnancies in any given year remains elusive, largely because of data collection gaps (NASEM, 2024a; Rossen et al., 2023). Pregnancy and childbirth are often relational experiences, with effects on not only the pregnant person but also partners, families, and communities.
Adverse pregnancy outcomes most often have multiple contributing factors, including genetic, epigenetic, environmental, and behavioral factors; quality of care; and structural causes. As with many health outcomes, inequities in pregnancy exist across and between multiple axes of social risk, including education, access to care, and geographic location. Data are limited on how structural drivers of health, such as racism, discrimination, classism, and sexism, manifest in the body to change biological process and impact pregnancy outcomes. However, epidemiologic data demonstrate that Black, American Indian and Alaska Native (AIAN), and Native Hawaiian and Pacific Islander (NHPI) mothers and infants, for example, experience two- to threefold higher rates of adverse outcomes compared to their White counterparts (CDC, n.d.-c; Hill et al., 2022; NASEM, 2020; Petersen et al., 2019). The gaps in these outcomes, which include stillbirth, low birthweight, infant mortality, and maternal mortality, have remained nearly unchanged for over a century despite medical, technical, and public health advances that have reduced overall rates. This suggests that structural factors—in this case, structural racism—play a role in distributing access to opportunities for health improvement inequitably across social axes (Hill et al., 2022; NASEM, 2019, 2020, 2023).
This section provides examples of pregnancy-related conditions for which research investment could significantly improve treatment and prevention or close gaps in maternal health morbidity and mortality. For many
of these conditions, different pathophysiologic pathways may lead to the same downstream consequences, but current scientific knowledge lacks the detail and precision to differentiate these, which also results in ineffective treatments, as heterogenous processes are often lumped together and treated similarly.
Maternal Mortality
Maternal mortality is generally defined as death while pregnant or within 42 days of the end of the pregnancy, and the Centers for Disease Control and Prevention (CDC) use the phrase “pregnancy-related mortality” to include deaths that occur during or within 1 year of the end of pregnancy from any cause related to or aggravated by the pregnancy (CDC, n.d.-b; WHO, n.d.). In 2022, 817 people died of pregnancy-related causes in the United States, resulting in a maternal mortality ratio of 22 per 100,000 live births (Hoyert, 2024). This has earned the United States the unenviable rank of the highest maternal mortality ratio among high-income countries (Gunja et al., 2024).6 Its maternal mortality is also characterized by stark racial disparities, with NHPI, Black, and AIAN people having the highest rates (CDC, n.d.-b). In 2022, the rate was 49.5 per 100,000 live births among Black patients, which is nearly threefold higher than the 19 per 100,000 among White birthing people (Hoyert, 2024). Geographical disparities also exist, with the highest rates in Arkansas and Mississippi (CDC, n.d.-a).
A review of maternal deaths from 2017 to 2019 in 36 states showed that pregnancy-related deaths occurred during pregnancy, birth, and up to 1 year postpartum, with 53 percent occurring from 7 days to 1 year postpartum (Trost et al., 2022). Moreover, over 80 percent of these deaths were determined to be preventable (Trost et al., 2022).
The etiology of maternal mortality is multifaceted and includes direct and indirect causes. The CDC analysis showed that the six most frequent direct causes were mental health conditions (22.7 percent), hemorrhage (13.7 percent), cardiac and coronary conditions (12.8 percent), infection (9.2 percent), thrombotic embolism (8.7 percent), and cardiomyopathy (8.5 percent), accounting for over 75 percent of these deaths (Trost et al., 2022). The leading underlying cause of death varied by race and ethnicity, with cardiac and coronary conditions most common among non-Hispanic Black persons; mental health conditions most common among Hispanic and non-Hispanic White persons; and hemorrhage most common among non-Hispanic Asian people (Trost et al., 2022).
___________________
6 High-income countries have data collection, reporting, definitional, and population differences, making this comparison complex.
Indirect causes of maternal mortality include structural racism, economic inequities, public policies, such as a lack of access to insurance or parental leave, and other social drivers, including food, housing, and transportation instability, that culminate in inequities in the longitudinal provision of preconception, antenatal, intrapartum, and postpartum care at the system, provider, and patient levels (Crear-Perry et al., 2021; Howell, 2018). The effect of state abortion bans enabled by the Supreme Court overturning Roe v. Wade may also affect maternal deaths. There have numerous reports and litigation on the effect of the denial of care that includes abortion or miscarriage management care to women experiencing potentially life-threatening pregnancy-related emergencies (Grossman et al., 2023).7,8,9 Research conducted before the Dobbs v. Jackson Women’s Health Organization decision found a higher likelihood of maternal mortality in states with restrictive abortion policies (Vilda et al., 2021). Recent news reports have begun to identify cases of maternal deaths that have been attributed to denial of appropriate care due to abortion bans, but initial research from national vital statistics data for the year following the decision has not noted such an effect (Stevenson and Root, 2024; Surana, 2024a,b). A landmark prospective study on the effect of abortion denial found that women who were denied abortions and who gave birth had higher rates of pregnancy-related complications, including, eclampsia, postpartum hemorrhage, and gestational hypertension, compared to those who were able to obtain a wanted abortion (ANSIRH, n.d.; Gerdts et al., 2016; Ralph et al., 2019).
Gaps in maternal mortality and morbidity research include difficulties in case ascertainment for maternal mortality from death records and potential misclassification in current coding methods and systems (Collier and Molina, 2019; Joseph et al., 2024; MacDorman and Declercq, 2018; van den Akker et al., 2017). Each U.S. state may choose to participate in Maternal Mortality Review Committee efforts; a multidisciplinary committee reviews the circumstances of maternal deaths to adjudicate pregnancy relatedness and opportunities for prevention or intervention (Collier and Molina, 2019; St. Pierre et al., 2018). Funding for this remains limited, as does the ability for any central authority to combine and synthesize recommendations for prevention or intervention to develop programs to reduce maternal mortality and morbidity (St. Pierre et al., 2018). In addition, granular analyses that provide insight into community or population experience are hampered by low numbers (e.g., lack of granular race data for NHPI individuals) (Trost et al., 2022).
___________________
7 Blackmon v. State of Tennessee (2023).
8 Adkins v. State of Idaho (2023).
9 Zurawski v. State of Texas (2023).
A leading cause of maternal mortality is death from suicide or overdose—that is, perinatal mental health concerns and substance use disorders (Chin et al., 2022; Han et al., 2024). Though a monitoring framework for maternal morbidity—a harbinger of problems that, if left unchecked, could lead to maternal mortality—exists and has been validated, no similar measure of severe maternal mental health morbidity exists to help identify and target those most at risk for suicide or overdose in the peripartum period.
As noted, indirect causes of maternal mortality are important contributors, so studies that focus on the social and structural determinants of health and their effect on maternal outcomes are needed (Crear-Perry et al., 2021). Gaps also remain in understanding provider access, availability, knowledge, and potential for bias in care around maternal mortality, particularly for acute health events (Howell, 2018; NASEM, 2021; Slaughter-Acey et al., 2023).
RPL
The definition of RPL differs across professional societies.10 Based on these varying definitions, 1–5 percent of individuals attempting pregnancy will experience it, and fewer than 1 percent will experience three or more consecutive first-trimester pregnancy losses (ACOG, 2024; Practice Committee of the American Society for Reproductive Medicine, 2012; Regan et al., 2023).
While embryonic aneuploidy, or abnormal chromosome number, is the most common cause of any one pregnancy loss, its contribution decreases as consecutive pregnancy losses increase. Other potential explanations include uterine anomalies, endocrine disorders, immune disorders, and thrombophilias, which are genetic or acquired blood clotting disorders (Ford and Schust, 2009; Regan et al., 2023). RPL confers significant mental, emotional, and financial burdens that affect health care costs, personal and family stress, and work productivity (Laijawala, 2024; Quenby et al., 2021). Despite these burdens, it remains unexplained in 50 percent of cases (ACOG, 2024; Ford and Schust, 2009). Furthermore, no treatments have consistently demonstrated effectiveness in maintaining pregnancies afterward. This is true even for interventions, including uterine septum resection and PG supplementation, aimed at specific relevant etiologies (Ford and Schust, 2009; Regan et al., 2023).
___________________
10 The American College of Obstetricians and Gynecologists, for example, defines RPL as having two or more miscarriages, while the American Society of Reproductive Medicine defines it as the loss of two or more clinical and consecutive pregnancies with either ultrasound or histopathological documentation, excluding ectopic and molar pregnancies, and the Royal College of Obstetricians and Gynecologists defines it as three or more consecutive first trimester miscarriages (ACOG, 2024; Practice Committee of the American Society for Reproductive Medicine, 2013; Regan et al., 2023).
Recent early trials for subsets of the RPL population have shown some promise. For example, intravenous immunoglobulin IVIG for individuals who have experienced more than four losses and PG supplementation for individuals with more than three losses and vaginal bleeding in the first trimester of a subsequent pregnancy may show promise for these small subsets, but their evidence base and effectiveness in practice remains under investigation given the lack of large-scale, randomized controlled trials and conclusive evidence (ACOG, 2021; Banjar et al., 2023; Coomarasamy et al., 2019, 2020; D’Mello et al., 2021; Habets et al., 2022; Shi et al., 2022; Yamada et al., 2022).
The failure of many proposed treatment strategies is likely due to several heterogenous disease processes that result in a similar clinical phenotype of RPL. Therefore, the entire relevant translational research spectrum would benefit from increased attention; it serves as a clear example of gaps in basic science knowledge. Understanding is limited of the processes that support appropriate implantation and permit early pregnancies to progress when the embryo has normal genes. This inadequate understanding of pathophysiology across both identified and yet-to-be-identified causes of RPL has generally hampered progress toward interventions that could mitigate the substantial emotional, financial, and potential long-term health burdens (Laijawala, 2024; Quenby et al., 2021).
Preeclampsia
Preeclampsia is on a spectrum of hypertensive diseases in pregnancy and affects 2–8 percent of all pregnant people globally (ACOG, n.d.). Classically, pregnant people are diagnosed when they exhibit new-onset elevated blood pressures and proteinuria, or elevated protein in the urine, beyond 20 weeks of pregnancy. More severe forms manifest with pulmonary edema, cardiomyopathy, seizures, uncontrolled headaches, or end-organ damage, such as acute liver or kidney injury. Preeclampsia and other related hypertensive disorders of pregnancy significantly affect maternal and fetal health, with more than 7 percent of maternal deaths stemming from preeclampsia and its complications (CDC, 2022).
In addition, preeclampsia drives a significant proportion of preterm births (PTBs) resulting from the need to induce birth early for maternal safety and from small for gestational age neonates due to associated poor placental function. Black and African American pregnant people in the United States have a moderately increased risk of preeclampsia compared to White individuals and a higher likelihood of related morbidity and mortality, suggesting differences in treatment and care access (MacDorman et al., 2021; Zhang et al., 2020b). Preeclampsia confers lifelong increased cardiovascular risks that compound its health effects and underscore the urgency of understanding, treating, and preventing it and its long-term consequences.
The origins of preeclampsia are not fully understood but likely begin with impaired placental implantation (Dimitriadis et al., 2023; Huppertz, 2008; Kalafat and Thilaganathan, 2017; Kornacki et al., 2023). Advances in understanding the roles of serum markers that indicate dysfunction within the lining of small blood vessels and markers of immune system dysfunction have not yet translated into improved diagnostic or therapeutic options (Amaral et al., 2017; Dimitriadis et al., 2023; Jung et al., 2022). Preeclampsia remains a clinical diagnosis based on symptoms and signs consistent with it; diagnosis is challenging when other comorbidities exist that mimic these, such as chronic hypertension and autoimmune disease (Jung et al., 2022; Staff, 2019). The lack of a definitive diagnostic disease marker increases the potential for bias in interpreting the signs and symptoms by race, ethnicity, or other demographics, thereby increasing the possibility of inequitable outcomes (Dimitriadis et al., 2023; Johnson and Louis, 2022).
No treatments aside from delivery can slow, mitigate, or reverse the effects of preeclampsia (Bokuda and Ichihara, 2023; Dimitriadis et al., 2023; Magee et al., 2023; Staff, 2019). Despite promising results in animal models, trials of phosphodiesterase inhibitors and statins have failed to demonstrate effectiveness in humans; statins may reduce preterm, but not term, preeclampsia (Bokuda and Ichihara, 2023; Dimitriadis et al., 2023; Larré et al., 2018). A daily low-dose aspirin can decrease the likelihood of preeclampsia in individuals at risk, but clinicians continue to lack clarity around why it works, which dosage is most effective, or which population might benefit most (Dimitriadis et al., 2023). The lack of effective preventive and treatment options demonstrates the difficulty in bridging the wide chasm of clinical translation between basic science understanding and clinically meaningful diagnostic, preventive, and therapeutic outcomes. Given the broad effects, including the increased risk of serious conditions later in life, such as chronic hypertension, stroke, heart failure, heart attack, peripheral vascular disease, and kidney disease, and the role preeclampsia plays in inequities in maternal morbidity and mortality, a lagging understanding of diagnosis and treatment places pregnant people and their offspring at significant risk (Bokuda and Ichihara, 2023; Dimitriadis et al., 2023; Howell, 2018).
Gestational Diabetes (GD)
GD results from an inappropriate or dysregulated response to pregnancy-related decreases in insulin sensitivity. An imbalance in glucose intolerance and insulin production can lead to GD, but it remains unclear how the imbalance occurs or what hormones mediate the development of this disorder (Rassie et al., 2022).
Each year, 5–9 percent of U.S. pregnant individuals will develop GD, with an estimated annual cost of $1.6 billion related to additional antenatal
surveillance, such as ultrasounds and non-stress tests, and increased maternal, obstetric, and neonatal adverse outcomes (Bolduc et al., 2024; CDC, 2024a; Dall et al., 2019; Sweeting et al., 2024). It disproportionately affects Latina/Latine/Hispanic, NHPI, AIAN, and Asian (notably Asian Indian) people, contributing to an excess burden of perinatal morbidity (Greco et al., 2024; Gregory and Ely, 2022; Shah et al., 2021; Ye et al., 2022). In addition to increased rates, there are also gaps in glycemic control and disease outcomes among pregnant people of color, which might be attributable to lack of access to high-quality care, lack of culturally responsive treatments, and other structural barriers (Bower et al., 2019; CDC, 2023; Erbetta et al., 2022; Palatnik et al., 2022; Shah et al., 2021).
Approximately 20–60 percent of individuals diagnosed with GD will develop Type 2 diabetes in the next 10 years; for some, this results in a young age of onset, with a lifetime of managing a chronic illness and significant potential for cardiovascular, renal, neurologic, and cerebrovascular disease (Buchanan et al., 2012; Li et al., 2022). For individuals who develop Type 2 diabetes later in life, it remains unclear whether GD represents a manifestation of baseline risk for diabetes given the physiologic and hormonal challenges of pregnancy or itself somehow contributes to lifelong increased risk by permanently altering physiology. Recent genome-wide association studies have demonstrated some overlap between genes that increase susceptibility to Type 2 and GD, which provides some early insight into disease pathophysiology but cannot clarify the chronology of these events (Dalfrà et al., 2020).
GD is also associated with increases in adverse perinatal outcomes for birthing parent, fetus, and neonate, including cesarean birth; preeclampsia; shoulder dystocia, a condition where one or both shoulders of the baby become stuck during labor; fetal growth abnormalities, particularly macrosomia, or being oversized; neonatal hypoglycemia; stillbirth; and neonatal intensive care unit admission. Two large randomized controlled trials demonstrated that treating it results in reduced adverse perinatal outcomes, confirming observational studies suggesting that glycemic control reduces the risk of adverse outcomes (Crowther et al., 2005).
Research gaps in GD include understanding the hormonal physiology that contributes to both it and Type 2 diabetes risk and identifying the most effective screening windows, serum glucose thresholds for diagnostic tests, and implementation approaches to ensure all groups have access to high-quality and culturally responsive counseling and treatment.
Spontaneous PTB
PTB, or the birth of a live or stillborn infant before 37 weeks gestation, affects up 10 percent of U.S. pregnant people (CDC, 2024b; March
of Dimes, n.d.). The majority occurs at 32–36 weeks of pregnancy, and 70–80 percent of these are spontaneous and not as a result of medical intervention to induce birth (Goldenberg et al., 2008; March of Dimes, n.d.). The causes include spontaneous preterm labor (40–45 percent), premature rupture of membranes that cause amniotic fluid leaking before the onset of labor (25–30 percent), and, more rarely, premature dilation of the cervix (also known as “cervical insufficiency”) or placental abruption (premature separation of the placenta from the wall of the uterus) (Goldenberg et al., 2008). Approximately 20–30 percent of PTBs occur when clinicians decide to induce (medically or surgically) given a fetal or maternal complication that substantially increases the risk of ongoing pregnancy to the mother or fetus (Goldenberg et al., 2008; IOM, 2007). However, clinicians and investigators often cannot provide parents with clear reasons for their PTB experience, and many pregnant people feel responsible for the outcome, with associated feelings of guilt and shame.
The underlying processes that can prematurely trigger the labor cascade, resulting in spontaneous PTB, remain unclear (Goldenberg et al., 2008). This is a result, at least in part, to a poor understanding of the labor cascade itself; interventions for slowing or stopping the process in preterm, pathological situations have proven unsuccessful (Goldenberg et al., 2008; Iams et al., 2008; March of Dimes, 2020; Mayo Clinic, 2022).
Studies have demonstrated that inflammation, whether from microbial infection or an endogenous cause, plays a role in PTB (Goldenberg et al., 2008). However, how these abnormal inflammatory states begin—how maternal immune system tolerance for the fetus and vice versa becomes disrupted or dysfunctional—how and why infection may ascend into the uterus, and how the inflammatory milieu can trigger labor remains an area of investigation. In addition, multiple clinical and environmental factors, such as multifetal gestation, air pollution and heat exposure, stress, and others, have an association with PTB (Bekkar et al., 2020; Etzel, 2020; Goldenberg et al., 2008).
Preterm birth is a leading cause of neonatal morbidity and mortality worldwide, and inequities by race persist. Black and AIAN pregnant people’s risk of PTB exceeds that of White individuals by about 50 percent (Barreto et al., 2024; Raglan et al., 2016). It is also critical to consider the heterogeneity within racial and ethnic groups when addressing health equity (NASEM, 2023). Birth outcomes among Latino/a/x/e individuals are a salient example; although these outcomes are on average worse than for White pregnant patients, there is considerable variation. For example, in one study that included predominately Puerto Rican individuals, who have some of the highest rates of adverse outcomes, acculturation (measured by language preference and generation in the United States) was associated with higher gestational age and birthweight (Barcelona de Mendoza et al., 2016).
In addition to the immediate neonatal consequences, PTB also exposes mothers to increased cardiovascular complications and earlier all-cause mortality compared to individuals without a history of PTB (Crump et al., 2020; Wu et al., 2018).
Abortion
Even before the Supreme Court decision in Dobbs v. Jackson Women’s Health Organization,11 which overturned the federal right to abortion and protections for abortion access, data gaps surrounding abortion made it difficult to study. Reasons for data collection difficulty include the early gestation at which most abortions occur, concerns about criminalization of providers and patients, stigma, and the decentralized and siloed environments in which most abortion care takes place, with abortion clinics typically separated to greater or lesser degree from other health care institutions (NASEM, 2024d). As of August 2024, 14 states have banned abortion with limited and difficult to access exceptions, and an additional six states have limited it to early in pregnancy, often before people even know they are pregnant (KFF, 2024). The Guttmacher Institute estimates there were 1,037,000 abortions in the formal health care system in 2023, the first full year after the Supreme Court overturned Roe v. Wade (Maddow-Zimet and Gibson, 2024). This estimate does not include self-managed abortion, which has likely increased but presents even greater barriers to accurate measurement.
Despite the commonality of pregnancy termination, multiple data gaps exist (Gomez et al., 2024; NASEM, 2024d). These include the difficulty identifying which patients or communities might need abortion care but cannot access it, differences in health outcomes caused by delays in care, increased difficulties created by crossing state lines or accessing self-managed abortion resources, and a better understanding of the health implications of self-managed abortions in the present context of broader availability of mifepristone. There are also gaps in documenting changes in abortion access and delivery, understanding short- and long-term ramifications for restrictions, and implications for the workforce (Dennis, 2024).
There are numerous federal policy barriers and challenges to collecting abortion data and undertaking abortion-related research (NIH, n.d.-b,c; Schott et al., 2023). However, given the potential for significant effects of denied abortion and delays in miscarriage management interventions on maternal morbidity and mortality, and other important concerns affecting women’s health and well-being, abortion-related research is needed to protect women’s health and inform policy. In addition, post-Roe v. Wade
___________________
11 Dobbs v. Jackson Women’s Health Organization, 597 U.S. 215 (2022).
abortion bans have resulted in fewer medical residency applicants choosing to train in abortion-restrictive states; this could directly lead to worsening maternity care access and a negative impact on maternal health outcomes in those states (Orgera and Grover, 2024; Weiner, 2022).
Structural Barriers to Advancing Pregnancy Research
A chief barrier to pregnancy-related research is the prior designation of pregnant individuals as a vulnerable population for research safety. Vulnerable populations have social or medical circumstances that increase their susceptibility to coercion or inability to provide voluntary consent to research. Though pregnancy itself does not render people incapable of providing informed consent, the fetus was felt to be a third party who could not consent. Because of this designation, ethics boards most often required research procedures to have demonstrable direct benefit to both the pregnant person and fetus or direct benefit to the pregnant person and no more than minimal risk to the fetus. As discussed in Chapter 2, such barriers resulted in excluding pregnant and lactating individuals from nearly all protocols related to non-obstetric conditions or drug trials. Furthermore, the designation created a particularly high bar for risk tolerance in obstetric research. This has resulted in numerous fundamental questions remaining unanswered, such as the efficacy of certain drugs during pregnancy, safety of medication during lactation, or the pathophysiology of disorders in pregnancy (NASEM, 2024a).
While pregnant people received a new special populations designation by FDA in 2018, which removed some of the most restrictive rules, the significant knowledge gaps created by decades of treatment as a vulnerable population will take dedicated effort and funding to close. Furthermore, these rule changes have not sparked a dramatic increase in including pregnant and lactating individuals in trials (NASEM, 2024a). This has left them and their health care providers faced with the challenging task of determining which medications and vaccines are safe and effective and will affect their own health or that of their fetus or child. Conversely, some may choose to use these and face an unpredictable risk of harm and uncertain potential benefits. A 2024 National Academies report, Advancing Clinical Research with Pregnant and Lactating Populations: Overcoming Real and Perceived Liability Risks, recommends ways to improve the safe and ethical inclusion of pregnant and lactating people in clinical research, including recommending that NIH develop a plan to prioritize research with these populations across its ICs (NASEM, 2024a).
The structure and funding of NIH ICs also creates limitations for pregnancy-related research. The Eunice Kennedy Shriver National Institute for Child Health and Development (NICHD) is the only IC that specifically
includes pregnancy within its charge. However, it enters the NICHD purview largely as a driver of neonatal and infant health rather than an opportunity to understand either pregnancy itself or any maternal effects in the short and long terms. This results in researchers focusing questions and hypotheses from the frame of fetal and neonatal outcomes, leaving important maternal health–related questions understudied or unaddressed because of a lack of alignment with funding opportunities. The risk of becoming pregnant and the immediate and downstream consequences of pregnancy, labor, and birth on the body are unique. However, no permanent NIH infrastructure supports the research needed to advance scientific understanding of pregnancy and postpartum conditions to improve the health and well-being of people who are or capable of becoming pregnant and their families and address prevention (including contraception) to avoid pregnancies that are not desired or mistimed.
Summary of Maternal Disorders/Pregnancy-Related Complications
As demonstrated, researchers and clinicians have only the merest grasp of physiology, pathophysiology, and effective clinical treatments related to pregnancy and pregnancy-related disorders, a unifying thread within this research. In addition, data gaps hamper population health interventions and evidence-based policy making to prevent adverse pregnancy outcomes and close gaps by race, ethnicity, geography, or income. This situation stems from a lack of investment in research at the maternal–fetal interface and lack of research understanding and intervening on structural and policy barriers that have impeded progress.
DIFFERENTIAL EFFECT BY SEX AND INCREASED FEMALE DALYS RESULTING FROM DISABLING CONDITIONS
Mood Disorders (Depressive and Anxiety Disorders)
Depression affects women throughout their life course and includes conditions such as premenstrual dysphoric disorder, perinatal depression, and depression related to the menopause transition. Multiple studies have illustrated that depression is higher among women compared to men and among women of younger compared to older age (NASEM, 2024b). The prevalence of depression from 2015 to 2020 reported within the past year increased in both adolescent and adult women and men but was almost two times higher in women compared to men, at 11.8 percent versus 6.4 percent in 2020 (Goodwin et al., 2022). Although racially and ethnically minoritized women report a lower prevalence of depression, they report exhibiting distinct differences in presentation; for example, Black and Latina women
experience greater somatic symptoms compared to White women (Phimphasone-Brady et al., 2023). Postpartum depression, defined as symptoms occurring during pregnancy or in 4 weeks after birth, is 3.0–25.2 percent and higher among AIAN, Asian American and Pacific Islander, and non-Hispanic Black women compared to non-Hispanic White women (Bauman et al., 2020; NASEM, 2024b).
A 2024 National Academies report identified research gaps related to depression in women, such as the mechanisms that underlie sex differences (NASEM, 2024b). Additional models are also needed to better understand the molecular basis of hormonally driven vulnerability to depression. Research on sex hormone and gene interactions and how sex chromosome effects are involved in the pathophysiology of depression in women are also critical (NASEM, 2024b). The report also describes the gaps in research on inflammatory triggers for depression in women, such as trauma, adverse childhood experiences, and stress, that can inform therapy development. More studies on the bidirectional influences of depression and other chronic conditions and how depression manifests across the life course will help to address research gaps. A better understanding of environmental influences in the development of depression in women is also needed (NASEM, 2024b).
Research on factors that may make women more susceptible to depression and biopsychosocial factors, such as nutrition/nutrients, microbiome, lifestyle, that may counter it is needed. Other gaps include developing screening tools that delineate the diagnostic features of perinatal depression, postpartum depression, and major depressive disorder to better identify women at risk along with research to incorporate racial, ethnic, and cultural considerations into clinical trials to treat depression in women at all stages of the life cycle (NASEM, 2024b).
Anxiety disorders are reported to be more prevalent in women compared to men based on national data. They contributed to greater global DALYs in women compared to men both before and during the COVID-19 pandemic and led to an additional 9.05 million DALYs resulting from the pandemic, of which 6.11 million were attributed to women and 2.94 million to men (COVID-19 Mental Disorders Collaborators, 2021). In 2019, 19.0 percent of women compared to 11.9 percent of men in the United States experienced anxiety symptoms within the past 2 weeks (Terlizzi and Villarroel, 2020).
An analysis of pooled studies have found that the prevalence of anxiety disorders during pregnancy or postpartum was 20.7 percent (Fawcett et al., 2019). Sex differences are attributed to both biological and social factors, including experiencing greater stressors, such as childhood abuse and trauma, and the presence and interaction of the central nervous system with hormonal fluctuations during puberty, the menstrual cycle, pregnancy, and the menopause transition (Hantsoo and Epperson, 2017).
In general, research on anxiety disorders in women is lacking (Hantsoo and Epperson, 2017). Further research on improving screening across the life-span is needed, given the clear differences in presentation of anxiety between women and men, and to further understand the exact sex-specific and hormonal mechanisms for treatment considerations and development of pharmacological therapies (Hantsoo and Epperson, 2017; Li and Graham, 2017). Given significant unmet needs for mental health services specifically among Indigenous and Black women, strategies to mitigate disparities in treatment and outcomes are needed (Taiwo et al., 2024). The factors associated with anxiety in racially and ethnically minoritized women, especially during the menopause transition, are less understood. A recent scoping review identified that approaches to address treatment considerations through the use of health care services, intervention, and implementation science are needed (Lewis Johnson et al., 2024)
Osteoarthritis (OA)
Musculoskeletal disorders are among the conditions with highest DALY burden, especially among women. OA is discussed here; see Chapters 2 and 5 for information on osteoporosis, which is also more prevalent among women and, due to the fractures it causes via loss of bone mass, is associated with disability and mortality. OA is generally not present until after the age of 50. Knee OA (KOA) is one of the most disabling diseases among older people and more prevalent in females. During the menopause transition, when serum estrogen levels decline (and then stabilize at a lower level in postmenopause), females have nearly twice the odds of KOA, have higher prevalence after age 55, and are more likely to experience pain and disability compared with males of the same age (Silverwood et al., 2015; Srikanth et al., 2005). Despite the increasing evidence pointing toward a higher risk of KOA in females, sex is often used only as an adjustment factor, and studies rarely report sex-specific estimates.
Hand OA, which often becomes clinically active around the menopause transition and tends to be hereditary, affects females at nearly three times the rate of males. A recent study of 3,588 participants in the Osteoarthritis Initiative found complex differences by age, sex, and race, with increasing prevalence rates with older age in both females and males but rates of incident disease peaking in females at ages 55–64, whereas for males the increase is more gradual and peaks later in life (Eaton et al., 2022). Hip osteoarthritis (HOA) is also prevalent among older adults, and females report a greater prevalence of symptomatic HOA than males (Nelson et al., 2022). A population-based cohort study found that females were more likely than males to report hip symptoms (40 vs. 32 percent) at baseline
and to have symptomatic radiographic HOA (16 versus 12 percent) at the fourth follow-up (Nelson et al., 2022).
The etiology of sex differences in KOA, hand OA, and other sites of OA have not been thoroughly studied (Szilagyi et al., 2023). Certain risk factors, including body mass index, have been well documented in the literature, but more longitudinal studies are needed to examine sex differences in risk factors, including lifestyle, occupational, comorbidity, and environmental factors (Szilagyi et al., 2023). The role of estrogen and other hormonal deficiencies associated with the menopause transition and aging in contributing to these sex differences are also not understood. Identifying the risk factors and understanding the physiological differences that affect women more prominently could lead to better sex-specific preventive and treatment strategies (Segal et al., 2024). Furthermore, characterizing the burden of OA in racially and ethnically minoritized populations has been a challenge, with a need to standardize assessments of OA in these populations and provide estimates separately by sex (Nelson et al., 2022).
DIFFERENTIAL EFFECT BY SEX AND INCREASED FEMALE DALYS RESULTING FROM EARLY MORTALITY
Cardiometabolic Disease
Cardiometabolic diseases include conditions such as heart disease, heart failure, stroke, diabetes, and hypertension and contribute to significant morbidity and mortality in women. CVD was the leading cause of death among women in 2021, contributing to 439,729 deaths. In addition, heart disease was a significant cause of death, with 310,656 deaths reported in the same year (Martin et al., 2024). Stroke alone represented the fifth-leading cause of death in women and contributed to 92,038 deaths in 2021 (Martin et al., 2024). The lifetime risk of stroke is reported to be greater in women compared to men (Tsao et al., 2023). Premature deaths due to cardiometabolic disease have increased for women from 1999 to 2018, specifically for diabetes and cerebrovascular disease (Shah et al., 2020). Premature mortality disproportionately affects Black women; 27.4, 21.1, and 33.0 percent of deaths in 2018 were premature due to heart disease, cerebrovascular disease, and diabetes, respectively (Shah et al., 2020). The prevalence of CVD from 2017–2020 was highest in non-Hispanic Black women at 59 percent compared to 44.6 percent in non-Hispanic White, 37.3 percent in Hispanic, and 38.5 in non-Hispanic Asian women (Martin et al., 2024). CVD contributes to significant disparities in health outcomes, which are associated with diagnosing and treating CVD in women (Nguyen et al., 2024; Vogel et al., 2021).
The 2024 National Academies report Advancing Research on Chronic Conditions in Women identified research gaps related to cardiometabolic conditions in women (NASEM, 2024b). Specifically, the report calls for a better understanding of the molecular basis for the female-biased propensity to store fat, including through preclinical models. Additional research on gonadal hormone ablation in preclinical models throughout the life-span was also identified as necessary. The report also describes the need for human studies of new diabetes and obesity drugs and sodium glucose cotransporter 2 inhibitors on weight loss and long-term outcomes by sex and gender. Additional tools to support early and accurate diagnosis of CVD in women are also important to fill gaps in knowledge (NASEM, 2024b).
The report also discussed the need for standard diagnostic criteria for ischemia with no obstructive coronary artery disease and research to clarify mechanisms leading to both it and myocardial infarction with no obstructive coronary artery disease in women. No guidelines are available on the evaluation and treatment for spontaneous coronary artery dissection. Finally, disaggregated data on CVD in Hispanic/Latina, Asian American, and NHPI women are needed (NASEM, 2024b).
As noted, depression and anxiety are more common among women than men and are risk factors for developing cardiometabolic disorders, such as hypertension, diabetes, and hyperlipidemia, and adverse cardiometabolic events (Civieri et al., 2024; Mattina et al., 2019; Rome et al., 2022). A 2024 retrospective cohort study of more than 71,000 participants found that those with anxiety and/or depression were at significantly higher risk of developing new cardiometabolic risk factors within a shorter time even after adjustment for demographics and health behaviors; the greatest effect was among young women, potentially mediated by neuroimmune pathways related to stress, such as systemic, chronic inflammation and autonomic nervous system dysfunction (Civieri et al., 2024). In addition, a variety of sex-specific risk factors related to hormonal life course changes in menarche, fertility, pregnancy, breastfeeding, and the menopause transition alter women’s risk for cardiometabolic diseases (O’Kelly et al., 2022; Parikh et al., 2021). For example, a history of common adverse pregnancy outcomes, such as PTB, GD, and hypertensive disorders of pregnancy, increase a woman’s lifetime risk of cardiometabolic diseases, while lactation and breastfeeding decrease it. Although the American Heart Association recommended screening for adverse birth outcomes as a universal aspect of cardiometabolic risk assessment for women in their 2011 update, improvements in risk prediction have not followed (Bahr, 2016; Gladstone et al., 2019; Mosca et al., 2011). On the other hand, breastfeeding has been considered a protective factor for cardiometabolic health, for women both with and without hypertensive disorders of pregnancy (Magnus et al., 2023).
More research is needed to understand the mechanisms and pathways linking these sex-specific risk and protective factors for identification, prevention, and treatment of later cardiometabolic diseases related to reproductive health (O’Kelly et al., 2022).
DIFFERENTIAL EFFECT BY SEX AND INCREASED FEMALE DALYS RESULTING FROM DISABLING CONDITIONS AND EARLY MORTALITY
Autoimmune Disorders
Autoimmune disorders constitute 80–150 different conditions, and their overall prevalence is difficult to measure, given the lack of consensus in number (NASEM, 2022). The last comprehensive study of U.S. prevalence was in 2009, producing an estimate of 7.6–9.4 percent of the population; however, it only included 29 conditions, and the prevalence is likely underreported (Cooper et al., 2009; NASEM, 2022). A recent U.K. population-based cohort study of 19 autoimmune disorders found that 1 in 10 individuals had an autoimmune disorder, with almost two-thirds of those female and one-third male (Conrad et al., 2023). In the 2022 NASEM report Enhancing NIH Research on Autoimmune Disease, the committee points out that several autoimmune disorders are overrepresented in female patients, including Sjögren’s Disease, systemic lupus erythematosus, rheumatoid arthritis, multiple sclerosis (MS), celiac disease, and inflammatory bowel disease. The incidence and prevalence of some autoimmune disorders have increased and are associated with the co-occurrence of other chronic conditions.
National Academies reports issued in 2022 and 2024 outlined research gaps related to autoimmune disorders in women (NASEM, 2022, 2024b). The 2024 report, for example, identified the need for more research to understand how inflammatory and immune system pathways affect the development of chronic conditions in women (NASEM, 2024b). Research on MS, which primarily affects women, needs to examine how hormonal and sex chromosome mechanisms intersect. Research is also needed to understand how factors, particularly Epstein-Barr viral infection, body weight, and others may contribute to the development of MS (NASEM, 2024b).
The 2022 National Academies report identified additional research gaps, including the need for population-based surveillance and epidemiological data on autoimmune diseases and measures of autoimmunity. Data are needed on autoantibodies that can predict and diagnose autoimmune diseases; common mechanisms in inflammation; gene–environment interactions within and across these diseases; the role of environmental
exposures; and the effect of interventions to address the impact of comorbidities and complications for patients (NASEM, 2022). The report also identified the need for clinical and basic research to understand heterogeneity across and within autoimmune diseases and examine rare ones (NASEM, 2022).
Neurodegenerative Diseases, AD, and Dementias—Cognition Across the Life Course
Both sex and gender affect the etiology, presentation, and treatment outcomes of many neurological disorders. Ongoing research aims to examine the role of sex and gender on cognition in specific neurodegenerative conditions, such as Parkinson’s disease, Huntington’s disease (HD), frontotemporal disease, and AD.
Sex Differences in Non-AD Neurodegenerative Disorders
The literature from epidemiological and clinic-based studies have generally supported the finding of a greater prevalence and earlier age of onset of Parkinson’s disease in men compared to women (Elbaz et al., 2002). Research has also reported sex-specific patterns regarding cognitive function, with female patients generally reporting less cognitive impairment in some but not all studies (Bakeberg et al., 2021; Chen et al., 2021; Reekes et al., 2020); studies have found that female patients had better frontal executive memory, visual perception, and verbal memory performance (Curtis et al., 2019; Liu et al., 2015) and that the apolipoprotein (APOE) e4 genotype conferred poorer cognitive performance that was more pronounced in men (Tipton et al., 2021). However, another study found that lower baseline semantic fluency scores were associated with a faster decline in women but not men (Cholerton et al., 2018).
Although the literature does not typically report sex differences in HD, studies have shown sex differences in clinical expression, with female disease gene carriers presenting with worse motor, cognitive, and depressive symptoms compared to male carriers (Hentosh et al., 2021). Female patients, for example, performed worse on verbal fluency, the symbol digits modality test, and the Stroop Interference test compared to men.
Studies in patients with frontotemporal disorders, characterized by changes in the frontal and temporal lobes that often present with significant emotional, language, and behavioral disturbances, reported that sex differences influenced clinical presentation and cognitive function. Some studies have noted the behavioral variant to be more common in male patients, whereas female patients may present with primary progressive aphasia.
In the behavioral variant, female patients outperformed male patients in measures of executive function and had less neurobehavioral changes despite a higher level of frontal atrophy. Consistent with other neurodegenerative conditions, female patients with the behavioral variant have higher behavioral and executive reserve (Illán-Gala et al., 2021).
AD and AD-Related Dementias
AD causes one of the most common types of dementia in older adults, accounting for 60–80 percent of cases. It was the fifth leading cause of death among those 65 and older in 2021 in the United States, and of the 6.9 million affected, 4.2 million are women and 73 percent are 75 years or older (Alzheimer’s Association, 2024; Hebert et al., 2001). An additional 5–7 million people age 65 and older are thought to have mild cognitive impairment resulting from AD (Alzheimer’s Association, 2024). The number of individuals with AD is expected to increase more in women than men over the coming years, reflecting biological factors and the increased longevity for women (Alzheimer’s Association, 2024; Hebert et al., 2013).
Recent evidence does not fully support previous reports that the risk of developing AD or other dementias differs between men and women of the same age (Shaw et al., 2021). This suggests that risk differences could have resulted from survival or selection bias, with projected average survival rates varying between 1.1 and 8.5 years across studies and affected by multiple factors, including age at diagnosis, sex, behavioral features, dementia subtype, motor system involvement, and medical comorbidities (Brodaty et al., 2012).
Biological factors
The strongest genetic risk factor for late-onset AD remains the APOE genotype. APOE encodes the brain’s major cholesterol transporter and has three common alleles: e2, e3 and e4. APOE e4 is associated with an increased risk of developing AD compared to e2 and e3 genotypes (Liu et al., 2013), and each APOE e4 allele reduces the average age of symptom onset by a decade. Female carriers of APOE e4 are at a greater risk of developing AD than male carriers, particularly those aged 65–75 (Neu et al., 2017). One study found for people in their 60s and 70s, females with APOE e4 +/+ genotype had less functional decline in an immediate recall memory test with increasing age than females with other genotypes (APOE e4 +/- and APOE e4 -/-), whereas males with the APOE e4 +/+ genotype had the most memory decline than other genotypes (Anstey et al., 2021a,b). The reason for these sex differences remains unclear and warrants further investigation.
The risk of developing AD and related forms of dementia increases in patients with vascular risk factors (Barnes and Yaffe, 2011; Ritchie et al., 2015). The data regarding potential sex differences related to cardiovascular risk factors and cognitive decline and dementia are inconsistent. For example, males have a higher prevalence of vascular risk factors and conditions up to about the age of 80, although a recent study suggested that despite the higher prevalence of these conditions in midlife, female individuals with vascular risk factors were at the greatest risk of cognitive decline (Huo et al., 2022). This area warrants investigation.
Neuroimaging markers have also been reported to show sex differences, with the increased occurrence of white matter hyperintensities increasing with advanced age in females postmenopause compared to males or pre-menopausal females (Ossenkoppele et al., 2020). It is unclear what specific physiological aspect of menopause might be contributing to this observation, in part because of a lack of quality data collected around the menopausal transition. In addition, the potential psychosocial stressors associated with the menopause transition, which could differ based on age, race, ethnicity, or age of onset, are still not fully examined as potential mediators to changes in physical or cognitive function in many of these research investigations (Faleschini et al., 2022).
Non-biological factors
Multiple lifestyle, psychological, behavioral, and environmental factors have been associated with AD, and the relationships between many of these and dementia vary by sex and gender (Baumgart et al., 2015), though the mechanism by which they contribute to differences in AD risk remain elusive. Multiple studies suggest that sex modifies the association between physical activity and cognition. Older females undergoing aerobic training showed greater cognitive gains than older males (Barha et al., 2017a,b), and physical activity maintenance over 10 years predicted fewer declines in multiple cognitive domains among females compared to males (Barha et al., 2020). Another study showed a positive correlation between physical activity and cognitive processing speed for females but not males, and the APOE e4 genotype once again moderated these relationships only in females (Sundermann et al., 2016).
Sex differences in sleep disturbances are commonly seen with neuropsychiatric behavior symptoms (Sateia, 2014) and linked to late-life cognitive decline and AD (Bombois et al., 2010; Ju et al., 2014; Yaffe et al., 2011). Females are especially vulnerable to sleep disruption at or around the menopause transition, with many experiencing symptoms that fit the diagnosis of insomnia (Joffe et al., 2010). Postmenopausal females are three times more likely to experience obstructive sleep apnea than premenopausal women, but whether these sex differences in sleep disruption affect AD risk is still
an area of active investigation (Bixler et al., 2001; Ju et al., 2017; Rumble et al., 2023).
Psychological stressors, such as gender- and race-based discrimination, harassment, poverty, and caregiving, may contribute to gender differences in late-life cognitive health, but research has not elucidated the mechanisms by which they may affect cognitive function and decline differentially by sex (Aartsen et al., 2004; Norton et al., 2010; Vitaliano, 2010). For instance, researchers have hypothesized an intersectional relationship between caregiving and cognitive health. Factors such as poor overall health; mental health conditions, such as depression and anxiety; social isolation; and chronic stress from economic hardships—stemming from unpaid caregiving and changes in employment—may interact in a way that negatively impacts a caregiver’s brain and cognitive function. This interaction could lead to pathways involving inflammation and excessive cortisol, further diminishing cognitive health (Alzheimer’s Association, 2024; Norton et al., 2010; Vitaliano, 2010). Life course research demonstrates that childhood socioeconomic position is more strongly associated with the rate of later-life cognitive decline in women than in men and that formal education was the strong mediator of that relationship (Wolfova et al., 2021).
Collectively, these social factors can affect medical treatment and access to care and the patient’s experience of care. Further research is warranted to understand sex-specific responses to early-life socioeconomic stressors and their impact on biological and other pathways that underlie them, setting the stage for differences in cognitive reserve later in life. This research investment will lead to interventions that beneficially affect long-term cognitive outcomes for men and women (Hidalgo et al., 2019).
Implications of Sex Differences in Cognitive Assessment Tools and Biomarkers
Studies are limited regarding sex-specific norms for neurocognitive impairment. Studies have shown that when compared with men, women across the life-span have stronger performance in most cognitive domains. Thus, continued failure to account for sex and gender differences can lead to underdetection of cognitive impairment in women, which can delay diagnosis and compromise access to early interventions.
Researchers are investigating using neuroimaging and blood-based markers to predict risk for decline or dementia. Some neuroimaging studies report that female patients have higher levels of brain glucose metabolism and greater cortical thickness compared to male patients, while other studies of AD biomarkers in blood and cerebrospinal fluid note higher cerebrospinal fluid levels of total tau protein in female patients (Buckley et al., 2019; Mielke, 2020; Ossenkoppele et al., 2020;
Sundermann et al., 2016, 2020). More research is needed to assess sex differences among these biomarkers and examine the properties of these biomarkers in older, racially diverse populations.
CONCLUDING OBSERVATIONS
Many women’s health conditions and approaches are not detailed in this chapter—for example, complementary health and naturopathic approaches, such as those the NIH National Center for Complementary and Integrative Health supports to address conditions such as perinatal depression, opioid use disorder, anxiety, and pain management (NCCIH, 2021). However, based on the conditions and factors that were reviewed in Chapters 2, 5, 6, and 7, the committee identified significant gaps for WHR across the life course. These include a lack of understanding of basic female physiology, insufficient study of specific conditions, inattention to SDOH and health inequities on specific health outcomes that focus on women, and the need for research on the interaction of these factors. Addressing these gaps requires a concerted and coordinated effort to include more women in clinical trials, increase funding for WHR, and focus on both biological and social determinants of health. This research is vital to ensure that all women receive the care and treatment they need.
REFERENCES
AACR (American Association for Cancer Research). 2024. AACR cancer disparities progress report 2024. Philadelphia, PA: American Association for Cancer Research.
Aartsen, M. J., M. Martin, and D. Zimprich. 2004. Gender differences in level and change in cognitive functioning. Results from the Longitudinal Aging Study Amsterdam. Gerontology 50(1):35–38.
Aboseif, C., and P. Liu. 2022. Pelvic organ prolapse. In Statpearls. Treasure Island, FL: StatPearls Publishing.
ACOG (American College of Obstetricians and Gynecologists). n.d. Gestational Hypertension and Preeclampsia. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2020/06/gestational-hypertension-and-preeclampsia (accessed August 15, 2024).
ACOG. 2021. Practice bulletin 200: Early pregnancy loss. Washington, DC: Committee on Practice Bulletins—Gynecology, American College of Obstetricians and Gynecologists.
ACOG. 2024. FAQs: Repeated Miscarriages. https://www.acog.org/womens-health/faqs/repeated-miscarriages (accessed October 14, 2024).
Akre, S., K. Sharma, S. Chakole, and M. B. Wanjari. 2022. Recent advances in the management of polycystic ovary syndrome: A review article. Cureus 14(8):e27689.
Al-Hawary, S. I. S., E. A. M. Saleh, N. A. Mamajanov, N. S. Gilmanova, H. O. Alsaab, A. Alghamdi, S. A. Ansari, A. H. R. Alawady, A. H. Alsaalamy, and A. J. Ibrahim. 2023. Breast cancer vaccines; a comprehensive and updated review. Pathology—Research and Practice 249:154735.
Al Harbi, R., I. A. McNeish, and M. El-Bahrawy. 2021. Ovarian sex cord-stromal tumors: An update on clinical features, molecular changes, and management. International Journal of Gynecologic Cancer 31(2):161–168.
Alblooshi, S., M. Taylor, and N. Gill. 2023. Does menopause elevate the risk for developing depression and anxiety? Results from a systematic review. Australasian Psychiatry 31(2):165–173.
Allen, L. A., N. Shrikrishnapalasuriyar, and D. A. Rees. 2022. Long-term health outcomes in young women with polycystic ovary syndrome: A narrative review. Clinical Endocrinology 97(2):187–198.
Alzheimer’s Association. 2024. 2024 Alzheimer’s disease facts and figures. Special report: Mapping a better future for dementia care navigation. Chicago, IL: Alzheimer’s Association.
Amaral, L. M., K. Wallace, M. Owens, and B. LaMarca. 2017. Pathophysiology and current clinical management of preeclampsia. Current Hypertension Reports 19(8):61.
American Cancer Society. 2024a. Cancer facts & figures 2024. Atlanta, GA: American Cancer Society.
American Cancer Society. 2024b. Key Statistics for Breast Cancer. https://www.cancer.org/cancer/types/breast-cancer/about/how-common-is-breast-cancer.html (accessed August 14, 2024).
ANSIRH (Advancing New Standards in Reproductive Health). n.d. The Turnaway Study. https://www.ansirh.org/research/ongoing/turnaway-study (accessed August 15, 2024).
Anstey, K. J., L. Ehrenfeld, M. E. Mortby, N. Cherbuin, R. Peters, K. M. Kiely, R. Eramudugolla, and M. H. Huque. 2021a. Gender differences in cognitive development in cohorts of young, middle, and older adulthood over 12 years. Developmental Psychology 57(8):1403–1410.
Anstey, K. J., R. Peters, M. E. Mortby, K. M. Kiely, R. Eramudugolla, N. Cherbuin, M. H. Huque, and R. A. Dixon. 2021b. Association of sex differences in dementia risk factors with sex differences in memory decline in a population-based cohort spanning 20–76 years. Scientific Reports 11(1):7710.
Augustovski, F., L. D. Colantonio, J. Galante, A. Bardach, J. E. Caporale, V. Zárate, L. H. Chuang, A. Pichon-Riviere, and P. Kind. 2018. Measuring the benefits of healthcare: DALYs and QALYs—does the choice of measure matter? A case study of two preventive interventions. International Journal of Health Policy and Management 7(2):120–136.
Bae-Jump, V. 2024. Obesity-Driven Endometrial Cancer: Gaps and Barriers to Improving Outcomes. Presentation to the NASEM Committee on the Assessment of NIH Research on Women’s Health, Meeting 3 (March 7, 2024). https://www.nationalacademies.org/event/docs/D1E982F058D7054AE8307F645CDE60D49C6215FC49F6?noSaveAs=1 (accessed October 21, 2024).
Bahr, R. 2016. Why screening tests to predict injury do not work—and probably never will. . . : A critical review. British Journal of Sports Medicine 50(13):776–780.
Bakeberg, M. C., A. M. Gorecki, J. E. Kenna, A. Jefferson, M. Byrnes, S. Ghosh, M. K. Horne, S. McGregor, R. Stell, S. Walters, P. Chivers, S. J. Winter, F. L. Mastaglia, and R. S. Anderton. 2021. Differential effects of sex on longitudinal patterns of cognitive decline in Parkinson’s disease. Journal Neurology 268(5):1903–1912.
Banjar, S., E. Kadour, R. Khoudja, S. Ton-leclerc, C. Beauchamp, M. Beltempo, M. H. Dahan, P. Gold, I. Jacques Kadoch, W. Jamal, C. Laskin, N. Mahutte, S. L. Reinblatt, C. Sylvestre, W. Buckett, and G. Genest. 2023. Intravenous immunoglobulin use in patients with unexplained recurrent pregnancy loss. American Journal of Reproductive Immunology 90(2):e13737.
Barcelona de Mendoza, V., E. Harville, K. Theall, P. Buekens, and L. Chasan-Taber. 2016. Acculturation and adverse birth outcomes in a predominantly Puerto Rican population. Maternal and Child Health Journal 20(6):1151–1160.
Barha, C. K., J. C. Davis, R. S. Falck, L. S. Nagamatsu, and T. Liu-Ambrose. 2017a. Sex differences in exercise efficacy to improve cognition: A systematic review and meta-analysis of randomized controlled trials in older humans. Frontiers in Neuroendocrinology 46:71–85.
Barha, C. K., G. R. Hsiung, J. R. Best, J. C. Davis, J. J. Eng, C. Jacova, P. E. Lee, M. Munkacsy, W. Cheung, and T. Liu-Ambrose. 2017b. Sex difference in aerobic exercise efficacy to improve cognition in older adults with vascular cognitive impairment: Secondary analysis of a randomized controlled trial. Journal of Alzheimer’s Disease 60(4):1397–1410.
Barha, C. K., J. R. Best, C. Rosano, K. Yaffe, J. M. Catov, and T. Liu-Ambrose. 2020. Sex-specific relationship between long-term maintenance of physical activity and cognition in the Health ABC study: Potential role of hippocampal and dorsolateral prefrontal cortex volume. Journals of Gerontology, Series A 75(4):764–770.
Barnard, M. E., L. V. Farland, B. Yan, J. Wang, B. Trabert, J. A. Doherty, H. D. Meeks, M. Madsen, E. Guinto, L. J. Collin, K. A. Maurer, J. M. Page, A. C. Kiser, M. W. Varner, K. Allen-Brady, A. Z. Pollack, K. R. Peterson, C. M. Peterson, and K. C. Schliep. 2024. Endometriosis typology and ovarian cancer risk. JAMA 332(6):482–489.
Barnes, D. E., and K. Yaffe. 2011. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurology 10(9):819–828.
Barreto, A., B. Formanowski, M.-M. Peña, E. G. Salazar, S. C. Handley, H. H. Burris, R. Ortiz, S. A. Lorch, and D. Montoya-Williams. 2024. Preterm birth risk and maternal nativity, ethnicity, and race. JAMA Network Open 7(3):e243194.
Bauman, B. L., J. Y. Ko, S. Cox, D. V. D’Angelo Mph, L. Warner, S. Folger, H. D. Tevendale, K. C. Coy, L. Harrison, and W. D. Barfield. 2020. Vital signs: Postpartum depressive symptoms and provider discussions about perinatal depression—United States, 2018. MMWR 69(19):575–581.
Baumgart, M., H. M. Snyder, M. C. Carrillo, S. Fazio, H. Kim, and H. Johns. 2015. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s & Dementia 11(6):718–726.
Bekkar, B., S. Pacheco, R. Basu, and N. DeNicola. 2020. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the U.S.: A systematic review. JAMA Network Open 3(6):e208243.
Berek, J. S., M. Renz, S. Kehoe, L. Kumar, and M. Friedlander. 2021. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update. International Journal of Gynecology & Obstetrics 155(S1):61–85.
Bixler, E. O., A. N. Vgontzas, H. M. Lin, T. Ten Have, J. Rein, A. Vela-Bueno, and A. Kales. 2001. Prevalence of sleep-disordered breathing in women: Effects of gender. American Journal of Respiratory and Critical Care Medicine 163(3 Pt 1):608–613.
Bokuda, K., and A. Ichihara. 2023. Preeclampsia up to date—what’s going on? Hypertension Research 46(8):1900–1907.
Bolduc, M. L. F., C. I. Mercado, Y. Zhang, E. A. Lundeen, N. D. Ford, K. M. Bullard, and D. C. Carty. 2024. Gestational diabetes prevalence estimates from three data sources, 2018. Maternal and Child Health Journal 28(8):1308–1314.
Bombois, S., P. Derambure, F. Pasquier, and C. Monaca. 2010. Sleep disorders in aging and dementia. Journal of Nutrition, Health and Aging 14(3):212–217.
Bower, J. K., B. N. Butler, S. Bose-Brill, J. Kue, and C. L. Wassel. 2019. Racial/ethnic differences in diabetes screening and hyperglycemia among U.S. women after gestational diabetes. Preventing Chronic Disease 16:E145.
Bozdag, G., S. Mumusoglu, D. Zengin, E. Karabulut, and B. O. Yildiz. 2016. The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Human Reproduction 31(12):2841–2855.
Brodaty, H., K. Seeher, and L. Gibson. 2012. Dementia time to death: A systematic literature review on survival time and years of life lost in people with dementia. International Psychogeriatrics 24(7):1034–1045.
Bromberger, J. T., and C. N. Epperson. 2018. Depression during and after the perimenopause: Impact of hormones, genetics, and environmental determinants of disease. Obstetrics and Gynecology Clinics of North America 45(4):663–678.
Buchanan, T. A., A. H. Xiang, and K. A. Page. 2012. Gestational diabetes mellitus: Risks and management during and after pregnancy. Nature Reviews Endocrinology 8(11):639–649.
Buck Louis, G. M., M. L. Hediger, C. M. Peterson, M. Croughan, R. Sundaram, J. Stanford, Z. Chen, V. Y. Fujimoto, M. W. Varner, A. Trumble, and L. C. Giudice. 2011. Incidence of endometriosis by study population and diagnostic method: The Endo study. Fertility and Sterility 96(2):360–365.
Buckley, R. F., E. C. Mormino, J. S. Rabin, T. J. Hohman, S. Landau, B. J. Hanseeuw, H. I. L. Jacobs, K. V. Papp, R. E. Amariglio, M. J. Properzi, A. P. Schultz, D. Kirn, M. R. Scott, T. Hedden, M. Farrell, J. Price, J. Chhatwal, D. M. Rentz, V. L. Villemagne, K. A. Johnson, and R. A. Sperling. 2019. Sex differences in the association of global amyloid and regional tau deposition measured by positron emission tomography in clinically normal older adults. JAMA Neurology 76(5):542–551.
Bulun, S. 2016. Physiology and pathology of the female reproductive axis. In Williams Textbook of Endocrinology, 13th ed., edited by S. Melmed, K. S. Polonsky, P. R. Larsen, and H. M. Kronenberg. Philadelphia, PA: Elsevier Health Sciences. Pp. 589–663.
Buys, S. S., E. Partridge, A. Black, C. C. Johnson, L. Lamerato, C. Isaacs, D. J. Reding, R. T. Greenlee, L. A. Yokochi, B. Kessel, E. D. Crawford, T. R. Church, G. L. Andriole, J. L. Weissfeld, M. N. Fouad, D. Chia, B. O’Brien, L. R. Ragard, J. D. Clapp, J. M. Rathmell, T. L. Riley, P. Hartge, P. F. Pinsky, C. S. Zhu, G. Izmirlian, B. S. Kramer, A. B. Miller, J.-L. Xu, P. C. Prorok, J. K. Gohagan, and C. D. Berg, for the PLCO Project Team. 2011. Effect of screening on ovarian cancer mortality: The Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening randomized controlled trial. JAMA 305(22):2295–2303.
Byatt, N., T. A. Simas, R. S. Lundquist, J. V. Johnson, and D. M. Ziedonis. 2012. Strategies for improving perinatal depression treatment in North American outpatient obstetric settings. Journal of Psychosomatic Obstetrics and Gynecology 33(4):143–161.
CDC (Centers for Disease Control and Prevention). n.d.-a. Maternal Deaths and Mortality Rates: Each State, the District of Columbia, United States, 2018–2022. https://www.cdc.gov/nchs/maternal-mortality/mmr-2018-2022-state-data.pdf (accessed August 26, 2024).
CDC. n.d.-b. Pregnancy Mortality Surveillance System. https://www.cdc.gov/maternal-mortality/php/pregnancy-mortality-surveillance/index.html (accessed August 14, 2024).
CDC. n.d.-c. Working Together to Reduce Black Maternal Mortality. https://www.cdc.gov/womens-health/features/maternal-mortality (accessed August 14, 2024).
CDC. 2022. Four in 5 Pregnancy-Related Deaths in the U.S. Are Preventable. https://www.cdc.gov/media/releases/2022/p0919-pregnancy-related-deaths.html (accessed August 16, 2024).
CDC. 2023. Quickstats: Percentage of mothers with gestational diabetes, by maternal age—National Vital Statistics System, United States, 2016 and 2021. MMWR 72(16).
CDC. 2024a. About Gestational Diabetes. https://www.cdc.gov/diabetes/about/gestational-diabetes.html (accessed October 20, 2024).
CDC. 2024b. Preterm Birth. https://www.cdc.gov/maternal-infant-health/preterm-birth/index.html (accessed October 22, 2024).
CDMRP. 2024. Ovarian Cancer. https://cdmrp.health.mil/ocrp/ (accessed August 16, 2024).
CDMRP. n.d. Ovarian Cancer Research Program: Strategic Plan. Fort Detrick, MD: Congressionally Directed Medical Research Porgrams.
Cetin, E., A. Al-Hendy, and M. Ciebiera. 2020. Non-hormonal mediators of uterine fibroid growth. Current Opinions in Obstetrics and Gynecology 32(5):361–370.
Che, Y., J. Yu, Y. S. Li, Y. C. Zhu, and T. Tao. 2023. Polycystic ovary syndrome: Challenges and possible solutions. Journal of Clinical Medicine 12(4).
Chen, M.-L., C.-H. Tan, H.-C. Su, P.-S. Sung, C.-Y. Chien, and R.-L. Yu. 2021. The impact of sex on the neurocognitive functions of patients with Parkinson’s disease. Brain Sciences 11(10):1331.
Chin, K., A. Wendt, I. M. Bennett, and A. Bhat. 2022. Suicide and maternal mortality. Current Psychiatry Reports 24(4):239–275.
Cholerton, B., C. O. Johnson, B. Fish, J. F. Quinn, K. A. Chung, A. L. Peterson-Hiller, L. S. Rosenthal, T. M. Dawson, M. S. Albert, S. C. Hu, I. F. Mata, J. B. Leverenz, K. L. Poston, T. J. Montine, C. P. Zabetian, and K. L. Edwards. 2018. Sex differences in progression to mild cognitive impairment and dementia in Parkinson’s disease. Parkinsonism & Related Disorders 50:29–36.
Christ, J. P., and M. I. Cedars. 2023. Current guidelines for diagnosing PCOS. Diagnostics 13(6).
Civieri, G., S. Abohashem, S. S. Grewal, W. Aldosoky, I. Qamar, E. Hanlon, K. W. Choi, L. M. Shin, R. P. Rosovsky, S. C. Bollepalli, H. C. Lau, A. Armoundas, A. V. Seligowski, S. M. Turgeon, R. K. Pitman, F. Tona, J. H. Wasfy, J. W. Smoller, S. Iliceto, J. Goldstein, C. Gebhard, M. T. Osborne, and A. Tawakol. 2024. Anxiety and depression associated with increased cardiovascular disease risk through accelerated development of risk factors. JACC Advances 3(9):101208.
Clarke, M. A., S. S. Devesa, S. V. Harvey, and N. Wentzensen. 2019. Hysterectomy-corrected uterine corpus cancer incidence trends and differences in relative survival reveal racial disparities and rising rates of nonendometrioid cancers. Journal of Clinical Oncology 37(22):1895–1908.
Coleman, R. L., A. M. Oza, D. Lorusso, C. Aghajanian, A. Oaknin, A. Dean, N. Colombo, J. I. Weberpals, A. Clamp, G. Scambia, A. Leary, R. W. Holloway, M. A. Gancedo, P. C. Fong, J. C. Goh, D. M. O’Malley, D. K. Armstrong, J. Garcia-Donas, E. M. Swisher, A. Floquet, G. E. Konecny, I. A. McNeish, C. L. Scott, T. Cameron, L. Maloney, J. Isaacson, S. Goble, C. Grace, T. C. Harding, M. Raponi, J. Sun, K. K. Lin, H. Giordano, and J. A. Ledermann. 2017. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): A randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet 390(10106):1949–1961.
Coleman, R. L., G. F. Fleming, M. F. Brady, E. M. Swisher, K. D. Steffensen, M. Friedlander, A. Okamoto, K. N. Moore, N. E. Ben-Baruch, T. L. Werner, N. G. Cloven, A. Oaknin, P. A. DiSilvestro, M. A. Morgan, J.-H. Nam, C. A. Leath, S. Nicum, A. R. Hagemann, R. D. Littell, D. Cella, S. Baron-Hay, J. Garcia-Donas, M. Mizuno, K. Bell-McGuinn, D. M. Sullivan, B. A. Bach, S. Bhattacharya, C. K. Ratajczak, P. J. Ansell, M. H. Dinh, C. Aghajanian, and M. A. Bookman. 2019. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. New England Journal of Medicine 381(25):2403–2415.
Collier, A. Y., and R. L. Molina. 2019. Maternal mortality in the United States: Updates on trends, causes, and solutions. NeoReviews 20(10):e561–e574.
Conrad, N., S. Misra, J. Y. Verbakel, G. Verbeke, G. Molenberghs, P. N. Taylor, J. Mason, N. Sattar, J. J. V. McMurray, I. B. McInnes, K. Khunti, and G. Cambridge. 2023. Incidence, prevalence, and co-occurrence of autoimmune disorders over time and by age, sex, and socioeconomic status: A population-based cohort study of 22 million individuals in the U.K. Lancet 401(10391):1878–1890.
Coomarasamy, A., A. J. Devall, V. Cheed, H. Harb, L. J. Middleton, I. D. Gallos, H. Williams, A. K. Eapen, T. Roberts, C. C. Ogwulu, I. Goranitis, J. P. Daniels, A. Ahmed, R. Bender-Atik, K. Bhatia, C. Bottomley, J. Brewin, M. Choudhary, F. Crosfill, S. Deb, W. C. Duncan, A. Ewer, K. Hinshaw, T. Holland, F. Izzat, J. Johns, K. Kriedt, M. A. Lumsden, P. Manda, J. E. Norman, N. Nunes, C. E. Overton, S. Quenby, S. Rao, J. Ross, A. Shahid, M. Underwood, N. Vaithilingam, L. Watkins, C. Wykes, A. Horne, and D. Jurkovic. 2019. A randomized trial of progesterone in women with bleeding in early pregnancy. New England Journal of Medicine 380(19):1815–1824.
Coomarasamy, A., A. J. Devall, J. J. Brosens, S. Quenby, M. D. Stephenson, S. Sierra, O. B. Christiansen, R. Small, J. Brewin, T. E. Roberts, R. Dhillon-Smith, H. Harb, H. Noordali,
A. Papadopoulou, A. Eapen, M. Prior, G. C. Di Renzo, K. Hinshaw, B. W. Mol, M. A. Lumsden, Y. Khalaf, A. Shennan, M. Goddijn, M. van Wely, M. Al-Memar, P. Bennett, T. Bourne, R. Rai, L. Regan, and I. D. Gallos. 2020. Micronized vaginal progesterone to prevent miscarriage: A critical evaluation of randomized evidence. American Journal of Obstetrics and Gynecology 223(2):167–176.
Cooper, G. S., M. L. Bynum, and E. C. Somers. 2009. Recent insights in the epidemiology of autoimmune diseases: Improved prevalence estimates and understanding of clustering of diseases. Journal of Autoimmunity 33(3–4):197–207.
COVID-19 Mental Disorders Collaborators. 2021. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 398(10312):1700–1712.
Cox, E. Q., N. A. Sowa, S. E. Meltzer-Brody, and B. N. Gaynes. 2016. The perinatal depression treatment cascade: Baby steps toward improving outcomes. Journal of Clinical Psychiatry 77(9):1189–1200.
Crear-Perry, J., R. Correa-de-Araujo, T. Lewis Johnson, M. R. McLemore, E. Neilson, and M. Wallace. 2021. Social and structural determinants of health inequities in maternal health. Journal of Women’s Health 30(2):230–235.
Cronin, K. A., S. Scott, A. U. Firth, H. Sung, S. J. Henley, R. L. Sherman, R. L. Siegel, R. N. Anderson, B. A. Kohler, V. B. Benard, S. Negoita, C. Wiggins, W. G. Cance, and A. Jemal. 2022. Annual report to the nation on the status of cancer, part 1: National cancer statistics. Cancer 128(24):4251–4284.
Crowther, C. A., J. E. Hiller, J. R. Moss, A. J. McPhee, W. S. Jeffries, and J. S. Robinson. 2005. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. New England Journal of Medicine 352(24):2477–2486.
Crump, C., J. Sundquist, and K. Sundquist. 2020. Preterm delivery and long term mortality in women: National cohort and co-sibling study. BMJ 370:m2533.
Cuijpers, P., and E. Karyotaki. 2021. The effects of psychological treatment of perinatal depression: An overview. Archives of Women’s Mental Health 24(5):801–806.
Curtis, A. F., M. Masellis, R. Camicioli, H. Davidson, and M. C. Tierney. 2019. Cognitive profile of non-demented Parkinson’s disease: Meta-analysis of domain and sex-specific deficits. Parkinsonism & Related Disorders 60:32–42.
D’Mello, R. J., C.-D. Hsu, P. Chaiworapongsa, and T. Chaiworapongsa. 2021. Update on the use of intravenous immunoglobulin in pregnancy. NeoReviews 22(1):e7–e24.
Dagher, R. K., H. E. Bruckheim, L. J. Colpe, E. Edwards, and D. B. White. 2021. Perinatal depression: Challenges and opportunities. Journal of Women’s Health 30(2):154–159.
Dalfrà, M. G., S. Burlina, G. G. Del Vescovo, and A. Lapolla. 2020. Genetics and epigenetics: New insight on gestational diabetes mellitus. Frontiers in Endocrinology 11:602477.
Dall, T. M., W. Yang, K. Gillespie, M. Mocarski, E. Byrne, I. Cintina, K. Beronja, A. P. Semilla, W. Iacobucci, and P. F. Hogan. 2019. The economic burden of elevated blood glucose levels in 2017: Diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Diabetes Care 42(9):1661–1668.
de Wit, A. E., E. J. Giltay, M. K. de Boer, M. Nathan, A. Wiley, S. Crawford, and H. Joffe. 2021. Predictors of irritability symptoms in mildly depressed perimenopausal women. Psychoneuroendocrinology 126:105128.
Deligiannidis, K. M. 2024. Research Gaps in Perinatal Mental Health Disorders: Perinatal Depression. Presentation to the NASEM Committee on the Assessment of NIH Research on Women’s Health, Meeting 3 (March 7, 2024). https://www.nationalacademies.org/event/docs/D6302B045662CDB06C85FC9E9EADAE8BFCB02A394EC5?noSaveAs=1 (accessed October 21, 2024).
Dennett, C. C., and J. Simon. 2015. The role of polycystic ovary syndrome in reproductive and metabolic health: Overview and approaches for treatment. Diabetes Spectrum 28(2):116–120.
Dennis, A. 2024. Research Gaps in Family Planning. Presentation to the NASEM Committee on the Assessment of NIH Research on Women’s Health, Meeting 2 (March 7, 2024). https://www.nationalacademies.org/documents/embed/link/LF2255DA3DD1C41C0A42D3BEF0989ACAECE3053A6A9B/file/D34E83DA13AE295302AE8CB1F2E5AD52868CFD491120?noSaveAs=1 (accessed August 16, 2024).
Dimitriadis, E., D. L. Rolnik, W. Zhou, G. Estrada-Gutierrez, K. Koga, R. P. V. Francisco, C. Whitehead, J. Hyett, F. da Silva Costa, K. Nicolaides, and E. Menkhorst. 2023. Preeclampsia. Nature Reviews Disease Primers 9(1):8.
Early Breast Cancer Trialists’ Collaborative Group. 2015. Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 386(10001):1341–1352.
Eaton, C. B., L. F. Schaefer, J. Duryea, J. B. Driban, G. H. Lo, M. B. Roberts, I. K. Haugen, B. Lu, M. C. Nevitt, M. C. Hochberg, R. D. Jackson, C. K. Kwoh, and T. McAlindon. 2022. Prevalence, incidence, and progression of radiographic and symptomatic hand osteoarthritis: The Osteoarthritis Initiative. Arthritis & Rheumatology 74(6):992–1000.
Elbaz, A., J. H. Bower, D. M. Maraganore, S. K. McDonnell, B. J. Peterson, J. E. Ahlskog, D. J. Schaid, and W. A. Rocca. 2002. Risk tables for Parkinsonism and Parkinson’s disease. Journal of Clinical Epidemiology 55(1):25–31.
Ellis, K., D. Munro, and J. Clarke. 2022. Endometriosis is undervalued: A call to action. Frontiers in Global Women’s Health 3:902371.
Eltoukhi, H. M., M. N. Modi, M. Weston, A. Y. Armstrong, and E. A. Stewart. 2014. The health disparities of uterine fibroid tumors for African American women: A public health issue. American Journal of Obstetrics and Gynecology 210(3):194–199.
Erbetta, K., J. Almeida, and M. R. Waldman. 2022. Racial, ethnic and nativity inequalities in gestational diabetes mellitus: The role of racial discrimination. SSM Population Health 19:101176.
Etzel, R. A. 2020. Is the environment associated with preterm birth? JAMA Network Open 3(4):e202239.
Faleschini, S., H. Tiemeier, S. L. Rifas-Shiman, J. Rich-Edwards, H. Joffe, W. Perng, J. Shifren, J. E. Chavarro, M. F. Hivert, and E. Oken. 2022. Longitudinal associations of psychosocial stressors with menopausal symptoms and well-being among women in midlife. Menopause 29(11):1247–1253.
Fawcett, E. J., N. Fairbrother, M. L. Cox, I. R. White, and J. M. Fawcett. 2019. The prevalence of anxiety disorders during pregnancy and the postpartum period: A multivariate Bayesian meta-analysis. Journal of Clinical Psychiatry 80(4).
FDA (Food and Drug Administration). 2016. FDA Grants Accelerated Approval to New Treatment for Advanced Ovarian Cancer. https://www.fda.gov/news-events/press-announcements/fda-grants-accelerated-approval-new-treatment-advanced-ovarian-cancer (accessed August 26, 2024).
Ford, H. B., and D. J. Schust. 2009. Recurrent pregnancy loss: Etiology, diagnosis, and therapy. Reviews in Obstetrics and Gynecology 2(2):76–83.
GBD 2021 Diseases and Injuries Collaborators. 2024. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease study 2021. Lancet 403(10440):2133–2161.
Gerdts, C., L. Dobkin, D. G. Foster, and E. B. Schwarz. 2016. Side effects, physical health consequences, and mortality associated with abortion and birth after an unwanted pregnancy. Women’s Health Issues 26(1):55–59.
Gladstone, R. A., J. Pudwell, K. A. Nerenberg, S. A. Grover, and G. N. Smith. 2019. Cardiovascular risk assessment and follow-up of women after hypertensive disorders of pregnancy: A prospective cohort study. Journal of Obstetrics and Gynaecology Canada 41(8):1157–1167.e1151.
Gnanasegar, R., W. Wolfman, L. H. Galan, A. Cullimore, and A. K. Shea. 2024. Does menopause hormone therapy improve symptoms of depression? Findings from a specialized menopause clinic. Menopause 31(4):320–325.
Goldenberg, R. L., J. F. Culhane, J. D. Iams, and R. Romero. 2008. Epidemiology and causes of preterm birth. Lancet 371(9606):75–84.
Gomez, I., K. Diep, B. Frederiksen, U. Ranji, and A. Salganicoff. 2024. Abortion Experiences, Knowledge, and Attitudes Among Women in the U.S.: Findings from the 2024 KFF Women’s Health Survey. https://www.kff.org/womens-health-policy/issue-brief/abortion-experiences-knowledge-attitudes-among-u-s-women-2024-womens-health-survey/ (accessed August 16, 2024).
González-Martín, A., B. Pothuri, I. Vergote, R. D. Christensen, W. Graybill, M. R. Mirza, C. McCormick, D. Lorusso, P. Hoskins, G. Freyer, K. Baumann, K. Jardon, A. Redondo, R. G. Moore, C. Vulsteke, R. E. O’Cearbhaill, B. Lund, F. Backes, P. Barretina-Ginesta, A. F. Haggerty, M. J. Rubio-Pérez, M. S. Shahin, G. Mangili, W. H. Bradley, I. Bruchim, K. Sun, I. A. Malinowska, Y. Li, D. Gupta, and B. J. Monk. 2019. Niraparib in patients with newly diagnosed advanced ovarian cancer. New England Journal of Medicine 381(25):2391–2402.
Goodman, J. H. 2009. Women’s attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth 36(1):60–69.
Goodwin, R. D., L. C. Dierker, M. Wu, S. Galea, C. W. Hoven, and A. H. Weinberger. 2022. Trends in U.S. depression prevalence from 2015 to 2020: The widening treatment gap. American Journal of Preventive Medicine 63(5):726–733.
Greco, E., M. Calanducci, K. H. Nicolaides, E. V. H. Barry, M. S. B. Huda, and S. Iliodromiti. 2024. Gestational diabetes mellitus and adverse maternal and perinatal outcomes in twin and singleton pregnancies: A systematic review and meta-analysis. American Journal of Obstetrics and Gynecology 230(2):213–225.
Greenberg, P. E., A.-A. Fournier, T. Sisitsky, M. Simes, R. Berman, S. H. Koenigsberg, and R. C. Kessler. 2021. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). PharmacoEconomics 39(6):653–665.
Gregory, E. C., and D. M. Ely. 2022. Trends and characteristics in gestational diabetes: United States, 2016–2020. National Vital Statistics Report 71(3):1–15.
Grossman, D., C. Joffe, S. Kaller, K. Kimport, E. Kinsey, K. Lerma, N. Morris, and K. White. 2023. Care post-Roe: Documenting cases of poor-quality care since the Dobbs decision. San Francisco, CA: Advancing New Standards in Reproductive Health.
Guevara, L. Z., E. Myers, R. Spencer, L. Havrilesky, and H. Moss. 2023. Disparities in allocation of research funding for female reproductive cancers based on race-specific disease burden (015). Gynecologic Oncology 176:S12.
Gunja, M. Z., E. D. Gumas, R. Masitha, and L. C. Zephyrin. 2024. Insights into the U.S. maternal mortality crisis: An international comparison. New York: The Commonwealth Fund.
Habets, D. H. J., K. Pelzner, L. Wieten, M. E. A. Spaanderman, E. Villamor, and S. Al-Nasiry. 2022. Intravenous immunoglobulins improve live birth rate among women with underlying immune conditions and recurrent pregnancy loss: A systematic review and meta-analysis. Allergy, Asthma & Clinical Immunology 18(1):23.
Han, B., W. M. Compton, E. B. Einstein, E. Elder, and N. D. Volkow. 2024. Pregnancy and postpartum drug overdose deaths in the U.S. before and during the COVID-19 pandemic. JAMA Psychiatry 81(3):270–283.
Hantsoo, L., and C. N. Epperson. 2017. Anxiety disorders among women: A female lifespan approach. Focus 15(2):162–172.
Hebert, L. E., P. A. Scherr, J. J. McCann, L. A. Beckett, and D. A. Evans. 2001. Is the risk of developing Alzheimer’s disease greater for women than for men? American Journal of Epidemiology 153(2):132–136.
Hebert, L. E., J. Weuve, P. A. Scherr, and D. A. Evans. 2013. Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology 80(19):1778–1783.
Hellberg, S. N., L. Lundegard, T. A. Hopkins, K. A. Thompson, M. Kang, T. Morris, and C. E. Schiller. 2023. Psychological distress and treatment preferences among parents amidst the COVID-19 pandemic. Psychiatry Research Communications 3(2):100109.
Hentosh, S., L. Zhu, J. Patino, J. W. Furr, N. P. Rocha, and E. Furr Stimming. 2021. Sex differences in Huntington’s disease: Evaluating the Enroll-HD database. Movement Disorders Clinical Practice 8(3):420–426.
Hidalgo, V., M. M. Pulopulos, and A. Salvador. 2019. Acute psychosocial stress effects on memory performance: Relevance of age and sex. Neurobiology of Learning and Memory 157:48–60.
Hill, L., S. Artiga, and U. Ranji. 2022. Racial disparities in maternal and infant health: Current status and efforts to address them. San Francisco, CA: KFF.
Hinchcliff, E. M., E. M. Bednar, K. H. Lu, and J. A. Rauh-Hain. 2019. Disparities in gynecologic cancer genetics evaluation. Gynecologic Oncology 153(1):184–191.
Howell, E. A. 2018. Reducing disparities in severe maternal morbidity and mortality. Clinical Obstetrics and Gynecology 61(2):387–399.
Hoyert, D. 2024. Maternal Mortality Rates in the United States, 2022. https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2022/maternal-mortality-rates-2022.htm (accessed August 14, 2024).
Huddleston, H. G., E. G. Jaswa, K. B. Casaletto, J. Neuhaus, C. Kim, M. Wellons, L. J. Launer, and K. Yaffe. 2024. Associations of polycystic ovary syndrome with indicators of brain health at midlife in the CARDIA cohort. Neurology 102(4):e208104.
Huo, N., P. Vemuri, J. Graff-Radford, J. Syrjanen, M. Machulda, D. S. Knopman, C. R. Jack, Jr., R. Petersen, and M. M. Mielke. 2022. Sex differences in the association between midlife cardiovascular conditions or risk factors with midlife cognitive decline. Neurology 98(6):e623–e632.
Huppertz, B. 2008. Placental origins of preeclampsia: Challenging the current hypothesis. Hypertension 51(4):970–975.
Iams, J. D., R. Romero, J. F. Culhane, and R. L. Goldenberg. 2008. Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth. Lancet 371(9607):164–175.
IHME (Institute for Health Metrics and Evaluation). n.d.-a. GBD Results. https://vizhub.healthdata.org/gbd-results/ (accessed August 13, 2024).
IHME. n.d.-b. Global Burden of Disease 2021 Disease Injury, and Impairment Factsheets. https://www.healthdata.org/research-analysis/diseases-injuries/factsheets-overview/about-disease-injury-impairment (accessed October 18, 2024).
IHME. n.d.-c. Global Burden of Disease Study 2021 (GBD 2021) Disability Weights. https://ghdx.healthdata.org/record/ihme-data/gbd-2021-disability-weights (accessed August 28, 2024).
Illán-Gala, I., K. B. Casaletto, S. Borrego-Écija, E. M. Arenaza-Urquijo, A. Wolf, Y. Cobigo, S. Y. M. Goh, A. M. Staffaroni, D. Alcolea, J. Fortea, R. Blesa, J. Clarimon, M. F. Iulita, A. Brugulat-Serrat, A. Lladó, L. T. Grinberg, K. Possin, K. P. Rankin, J. H. Kramer, G. D. Rabinovici, A. Boxer, W. W. Seeley, V. E. Sturm, M. L. Gorno-Tempini, B. L. Miller, R. Sánchez-Valle, D. C. Perry, A. Lleó, and H. J. Rosen. 2021. Sex differences in the behavioral variant of frontotemporal dementia: A new window to executive and behavioral reserve. Alzheimer’s & Dementia Journal 17(8):1329–1341.
IOM (Institute of Medicine). 2007. Preterm birth: Causes, consequences, and prevention. Washington DC: The National Academies Press.
Jagsi, R. 2024. Lessons from Breast Cancer Research and Remaining Gaps. Presentation to the NASEM Committee on the Assessement of NIH Research on Women’s Health, Meeting 3 (March 7, 2024). https://www.nationalacademies.org/event/docs/D44D1CC8D876137F76CCDC62F785C004079114963A63?noSaveAs=1 (accessed October 21, 2024).
Jagsi, R., S. T. Hawley, K. A. Griffith, N. K. Janz, A. W. Kurian, K. C. Ward, A. S. Hamilton, M. Morrow, and S. J. Katz. 2017. Contralateral prophylactic mastectomy decisions in a population-based sample of patients with early-stage breast cancer. JAMA Surgery 152(3):274–282.
Joffe, H., A. Massler, and K. M. Sharkey. 2010. Evaluation and management of sleep disturbance during the menopause transition. Seminars in Reproductive Medicine 28(5):404–421.
Johnson, J. D., and J. M. Louis. 2022. Does race or ethnicity play a role in the origin, pathophysiology, and outcomes of preeclampsia? An expert review of the literature. American Journal of Obstetrics & Gynecology 226(2):S876–S885.
Joseph, K. S., S. Lisonkova, A. Boutin, G. M. Muraca, N. Razaz, S. John, Y. Sabr, W.-S. Chan, A. Mehrabadi, J. S. Brandt, E. F. Schisterman, and C. V. Ananth. 2024. Maternal mortality in the United States: Are the high and rising rates due to changes in obstetrical factors, maternal medical conditions, or maternal mortality surveillance? American Journal of Obstetrics & Gynecology 230(4):440.e441–440.e413.
Ju, Y.-E. S., B. P. Lucey, and D. M. Holtzman. 2014. Sleep and Alzheimer disease pathology—a bidirectional relationship. Nature Reviews Neurology 10(2):115–119.
Ju, Y.-E. S., S. J. Ooms, C. Sutphen, S. L. Macauley, M. A. Zangrilli, G. Jerome, A. M. Fagan, E. Mignot, J. M. Zempel, J. A. H. R. Claassen, and D. M. Holtzman. 2017. Slow wave sleep disruption increases cerebrospinal fluid amyloid-β levels. Brain 140(8):2104–2111.
Jung, E., R. Romero, L. Yeo, N. Gomez-Lopez, P. Chaemsaithong, A. Jaovisidha, F. Gotsch, and O. Erez. 2022. The etiology of preeclampsia. American Journal of Obstetrics and Gynecology 226(2, Supplement):S844–S866.
Kalafat, E., and B. Thilaganathan. 2017. Cardiovascular origins of preeclampsia. Current Opinion in Obstetrics and Gynecology 29(6):383–389.
Karlan, B. Y. 2024. Ovarian Cancer 2024: Knowledge Gaps and Barriers to Improving Outcomes. Presentation to the NASEM Committee on the Assessment of NIH Research on Women’s Health, Meeting 3 (March 7, 2024). https://www.nationalacademies.org/event/docs/DC0C4FBDCA3CD136898AEE4C97B2D38780CE6060245B?noSaveAs=1 (accessed October 21, 2024).
KFF. 2024. Abortion in the United States Dashboard. https://www.kff.org/womens-health-policy/dashboard/abortion-in-the-u-s-dashboard/ (accessed August 15, 2024).
Kornacki, J., O. Olejniczak, R. Sibiak, P. Gutaj, and E. Wender-Ożegowska. 2023. Pathophysiology of pre-eclampsia—two theories of the development of the disease. International Journal of Molecular Sciences 25(1).
Laijawala, R. A. 2024. Recurrent pregnancy loss: Immunological aetiologies and associations with mental health. Brain, Behavior, & Immunity—Health 41:100868.
Larré, A. B., F. Sontag, D. M. Pasin, N. Paludo, R. R. do Amaral, B. E. P. da Costa, and C. E. Poli-de-Figueiredo. 2018. Phosphodiesterase inhibition in the treatment of preeclampsia: What is new? Current Hypertension Reports 20(10):83.
Lewis Johnson, T., L. M. Rowland, M. S. Ashraf, C. T. Clark, V. M. Dotson, A. A. Livinski, and M. Simon. 2024. Key findings from mental health research during the menopause transition for racially and ethnically minoritized women living in the United States: A scoping review. Journal of Women’s Health 33(2):113–131.
Li, L., J. Ji, Y. Li, Y. Huang, J. Y. Moon, and K. R.S. 2022. Gestational diabetes, subsequent Type 2 diabetes, and food security status: National Health and Nutrition Examination Survey, 2007–2018. Preventing Chronic Disease 19.
Li, S. H., and B. M. Graham. 2017. Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiatry 4(1):73–82.
Liu, C.-C., T. Kanekiyo, H. Xu, and G. Bu. 2013. Apolipoprotein E and Alzheimer disease: Risk, mechanisms and therapy. Nature Reviews Neurology 9(2):106–118.
Liu, R., D. M. Umbach, S. D. Peddada, Z. Xu, A. I. Tröster, X. Huang, and H. Chen. 2015. Potential sex differences in nonmotor symptoms in early drug-naive Parkinson disease. Neurology 84(21):2107–2115.
MacDorman, M. F., and E. Declercq. 2018. The failure of United States maternal mortality reporting and its impact on women’s lives. Birth 45(2):105–108.
MacDorman, M. F., M. Thoma, E. Declcerq, and E. A. Howell. 2021. Racial and ethnic disparities in maternal mortality in the United States using enhanced vital records, 2016–2017. American Journal of Public Health 111(9):1673–1681.
Maddow-Zimet, I., and C. Gibson. 2024. Despite Bans, Number of Abortions in the United States Increased in 2023. https://www.guttmacher.org/2024/03/despite-bans-number-abortions-united-states-increased-2023 (accessed August 15, 2024).
Magee, L. A., D. Wright, A. Syngelaki, P. von Dadelszen, R. Akolekar, A. Wright, and K. H. Nicolaides. 2023. Preeclampsia prevention by timed birth at term. Hypertension 80(5):969–978.
Magnus, M. C., M. K. Wallace, J. R. Demirci, J. M. Catov, M. J. Schmella, and A. Fraser. 2023. Breastfeeding and later-life cardiometabolic health in women with and without hypertensive disorders of pregnancy. Journal of the American Heart Association 12(5):e026696.
Maki, P. M., S. G. Kornstein, H. Joffe, J. T. Bromberger, E. W. Freeman, G. Athappilly, W. V. Bobo, L. H. Rubin, H. K. Koleva, L. S. Cohen, and C. N. Soares. 2019. Guidelines for the evaluation and treatment of perimenopausal depression: Summary and recommendations. Journal of Women’s Health 28(2):117–134.
March of Dimes. n.d. A Profile of Prematurity in the United States. https://www.marchofdimes.org/peristats/reports/united-states/prematurity-profile (accessed October 22, 2024).
March of Dimes. 2020. Treatments for Preterm Labor. https://www.marchofdimes.org/find-support/topics/birth/treatments-preterm-labor (accessed October 22, 2024).
Marsh, E. E., G. Wegienka, and D. R. Williams. 2024. Uterine fibroids. JAMA 331(17):1492–1493.
Martin, S. S., A. W. Aday, Z. I. Almarzooq, C. A. M. Anderson, P. Arora, C. L. Avery, C. M. Baker-Smith, B. Barone Gibbs, A. Z. Beaton, A. K. Boehme, Y. Commodore-Mensah, M. E. Currie, M. S. V. Elkind, K. R. Evenson, G. Generoso, D. G. Heard, S. Hiremath, M. C. Johansen, R. Kalani, D. S. Kazi, D. Ko, J. Liu, J. W. Magnani, E. D. Michos, M. E. Mussolino, S. D. Navaneethan, N. I. Parikh, S. M. Perman, R. Poudel, M. Rezk-Hanna, G. A. Roth, N. S. Shah, M.-P. St-Onge, E. L. Thacker, C. W. Tsao, S. M. Urbut, H. G. C. Van Spall, J. H. Voeks, N.-Y. Wang, N. D. Wong, S. S. Wong, K. Yaffe, and L. P. Palaniappan, on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. 2024. 2024 heart disease and stroke statistics: A report of U.S. and global data from the American Heart Association. Circulation 149(8):e347–e913.
Mattina, G. F., R. J. Van Lieshout, and M. Steiner. 2019. Inflammation, depression and cardiovascular disease in women: The role of the immune system across critical reproductive events. Therapeutic Advances in Cardiovascular Disease 13:1753944719851950.
Mayo Clinic. 2022. Preterm Labor. https://www.mayoclinic.org/diseases-conditions/preterm-labor/diagnosis-treatment/drc-20376848 (accessed October 22, 2024).
Meltzer-Brody, S., H. Colquhoun, R. Riesenberg, C. N. Epperson, K. M. Deligiannidis, D. R. Rubinow, H. Li, A. J. Sankoh, C. Clemson, A. Schacterle, J. Jonas, and S. Kanes. 2018. Brexanolone injection in post-partum depression: Two multicentre, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet 392(10152):1058–1070.
Menon, U., A. Gentry-Maharaj, M. Burnell, N. Singh, A. Ryan, C. Karpinskyj, G. Carlino, J. Taylor, S. K. Massingham, M. Raikou, J. K. Kalsi, R. Woolas, R. Manchanda, R. Arora, L. Casey, A. Dawnay, S. Dobbs, S. Leeson, T. Mould, M. W. Seif, A. Sharma, K. Williamson, Y. Liu, L. Fallowfield, A. J. McGuire, S. Campbell, S. J. Skates, I. J. Jacobs, and M. Parmar. 2021. Ovarian cancer population screening and mortality after long-term follow-up in the U.K. Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet 397(10290):2182–2193.
Mielke, M. M. 2020. Consideration of sex differences in the measurement and interpretation of Alzheimer disease-related biofluid-based biomarkers. Journal of Applied Laboratory Medicine 5(1):158–169.
Moore, K., N. Colombo, G. Scambia, B.-G. Kim, A. Oaknin, M. Friedlander, A. Lisyanskaya, A. Floquet, A. Leary, G. S. Sonke, C. Gourley, S. Banerjee, A. Oza, A. González-Martín, C. Aghajanian, W. Bradley, C. Mathews, J. Liu, E. S. Lowe, R. Bloomfield, and P. DiSilvestro. 2018. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. New England Journal of Medicine 379(26):2495–2505.
Morrison, L., S. Loibl, and N. C. Turner. 2024. The CDK4/6 inhibitor revolution—a game-changing era for breast cancer treatment. Nature Reviews Clinical Oncology 21(2):89–105.
Mosca, L., E. J. Benjamin, K. Berra, J. L. Bezanson, R. J. Dolor, D. M. Lloyd-Jones, L. K. Newby, I. L. Piña, V. L. Roger, L. J. Shaw, D. Zhao, T. M. Beckie, C. Bushnell, J. D’Armiento, P. M. Kris-Etherton, J. Fang, T. G. Ganiats, A. S. Gomes, C. R. Gracia, C. K. Haan, E. A. Jackson, D. R. Judelson, E. Kelepouris, C. J. Lavie, A. Moore, N. A. Nussmeier, E. Ofili, S. Oparil, P. Ouyang, V. W. Pinn, K. Sherif, S. C. Smith, Jr., G. Sopko, N. Chandra-Strobos, E. M. Urbina, V. Vaccarino, and N. K. Wenger. 2011. Effectiveness-based guidelines for the prevention of cardiovascular disease in women—2011 update: A guideline from the American Heart Association. Circulation 123(11):1243–1262.
Nabi, M. Y., S. Nauhria, M. Reel, S. Londono, A. Vasireddi, M. Elmiry, and P. Ramdass. 2022. Endometriosis and irritable bowel syndrome: A systematic review and meta-analyses. Frontiers in Medicine 9:914356.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. Washington, DC: The National Academies Press.
NASEM. 2020. Birth settings in America: Outcomes, quality, access, and choice. Washington, DC: The National Academies Press.
NASEM. 2021. Advancing maternal health equity and reducing maternal morbidity and mortality: Proceedings of a workshop. Washington, DC: The National Academies Press.
NASEM. 2022. Enhancing NIH research on autoimmune disease. Washington, DC: The National Academies Press.
NASEM. 2023. Federal policy to advance racial, ethnic, and tribal health equity. Washington, DC: The National Academies Press.
NASEM. 2024a. Advancing clinical research with pregnant and lactating populations: Overcoming real and perceived liability risks. Washington, DC: The National Academies Press.
NASEM. 2024b. Advancing research on chronic conditions in women. Washington, DC: The National Academies Press.
NASEM. 2024c. Overview of research gaps for selected conditions in women’s health research at the National Institutes of Health: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press.
NASEM. 2024d. Reproductive health, equity, and society: Exploring data challenges and needs in the wake of the Dobbs v. Jackson women’s health organization decision: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press.
NCCID (National Collaborating Centre for Infectious Diseases). 2015. Understanding Summary Measures Used to Estimate the Burden of Disease: All About HALYs, DALYs and QALYs. https://nccid.ca/publications/understanding-summary-measures-used-to-estimate-the-burden-of-disease/ (accessed August 8, 2024).
NCCIH (National Center for Complementary and Integrative Health). 2021. NCCIH strategic plan FY 2021–2025: Mapping a pathway to research on whole person health. Bethesda, MD: National Center for Complementary and Integrative Health.
NCCN (National Comprehensive Cancer Network). 2024. NCCN guidelines for patients: Ovarian cancer. Plymouth Meeting, PA: National Comprehensive Cancer Network.
NCI (National Cancer Institute). n.d.-a. NCI Cervical Cancer “Last Mile” Initiative. https://prevention.cancer.gov/major-programs/nci-cervical-cancer-last-mile-initiative (accessed August 14, 2024).
NCI. n.d.-b. SEER Cancer Stat Facts: Cervical Cancer. https://seer.cancer.gov/statfacts/html/cervix.html (accessed October 20, 2024).
NCI. n.d.-c. SEER Cancer Stat Facts: Ovarian Cancer. https://seer.cancer.gov/statfacts/html/ovary.html (accessed October 20, 2024).
NCI. n.d.-d. SEER Cancer Stat Facts: Uterine Cancer. https://seer.cancer.gov/statfacts/html/corp.html (accessed July 15, 2024).
NCI. 2020. With Two FDA Approvals, Prostate Cancer Treatment Enters the PARP Era. https://www.cancer.gov/news-events/cancer-currents-blog/2020/fda-olaparib-rucaparib-prostate-cancer (accessed October 20, 2024).
NCI. 2024a. All Cancer Sites Combined: Recent Trends in SEER age-Adjusted Incidence Rates, 2000–2021. https://seer.cancer.gov/statistics-Network/explorer/application.html?site=1&data_type=1&graph_type=2&compareBy=sex&chk_sex_3=3&chk_sex_2=2&rate_type=2&race=1&age_range=1&hdn_stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2#resultsRegion0 (accessed August 21, 2024).
NCI. 2024b. Breast: Recent Trends in SEER Relative Survival Rates, 2000–2021: By Race/Ethnicity, 3-year Relative Survival, Female, All Ages, All Stages. https://seer.cancer.gov/statistics-network/explorer/application.html?site=55&data_type=4&graph_type=2&compareBy=race&chk_race_1=1&chk_race_3=3&chk_race_2=2&relative_survival_interval=3&sex=3&age_range=1&stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=1%23resultsRegion0 (accessed October 20, 2024).
NCI. 2024c. Cervix Uteri: Recent Trends in SEER Relative Survival Rates, 2000–2021: Female by Race/Ethnicity, 3-Year Relative Survival, All Ages, All Stages. https://seer.cancer.gov/statistics-network/explorer/application.html?site=57&data_type=4&graph_type=2&compareBy=race&chk_race_1=1&chk_race_3=3&chk_race_2=2&relative_survival_interval=3&hdn_sex=3&age_range=1&stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=1#resultsRegion0 (accessed October 20, 2024).
NCI. 2024d. Corpus and Uterus, Nos: Recent Trends in SEER Relative Survival Rates, 2000–2021: Female by Race/Ethnicty, 3-Year Relative Survival, All Ages, All Stages. https://seer.cancer.gov/statistics-network/explorer/application.html?site=58&data_type=4&graph_type=2&compareBy=race&chk_race_1=1&chk_race_3=3&chk_race_2=2&relative_survival_interval=3&hdn_sex=3&age_range=1&stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2#resultsRegion0 (accessed October 20, 2024).
NCI. 2024e. Funding for Research Areas. https://www.cancer.gov/about-nci/budget/fact-book/data/research-funding (accessed August 14, 2024).
NCI. 2024f. Ovary: Recent Trends in SEER Relative Survival Rates, 2000–2021: Female by Race/Ethnicity, 3-Year Relative Survival, All Ages, All Stages. https://seer.cancer.gov/statistics-network/explorer/application.html?site=61&data_type=4&graph_type=2&compareBy=race&chk_race_3=3&chk_race_2=2&relative_survival_interval=3&hdn_sex=3&age_range=1&stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2#resultsRegion0 (accessed August 21, 2024).
Nelson, A. E., D. Hu, L. Arbeeva, C. Alvarez, R. J. Cleveland, T. A. Schwartz, L. B. Murphy, C. G. Helmick, L. F. Callahan, J. B. Renner, J. M. Jordan, and Y. M. Golightly. 2022. Point prevalence of hip symptoms, radiographic, and symptomatic OA at five time points: The Johnston County Osteoarthritis Project, 1991–2018. Osteoarthritis and Cartilage Open 4(2).
Neu, S. C., J. Pa, W. Kukull, D. Beekly, A. Kuzma, P. Gangadharan, L. S. Wang, K. Romero, S. P. Arneric, A. Redolfi, D. Orlandi, G. B. Frisoni, R. Au, S. Devine, S. Auerbach, A. Espinosa, M. Boada, A. Ruiz, S. C. Johnson, R. Koscik, J. J. Wang, W. C. Hsu, Y. L. Chen, and A. W. Toga. 2017. Apolipoprotein E genotype and sex risk factors for Alzheimer disease: A meta-analysis. JAMA Neurology 74(10):1178–1189.
Nguyen, A. H., M. Hurwitz, S. A. Sullivan, A. Saad, J. L. W. Kennedy, and G. Sharma. 2024. Update on sex specific risk factors in cardiovascular disease. Frontiers in Cardiovascular Medicine 11:1352675.
NIA (National Institute on Aging). 2022. Research Highlights: Research Explores the Impact of Menopause on Women’s Health and Aging. https://www.nia.nih.gov/news/research-explores-impact-menopause-womens-health-and-aging (accessed October 21, 2024).
NIH (National Institutes of Health). n.d.-a. Improving Health: Cancer. https://www.nih.gov/about-nih/what-we-do/impact-nih-research/improving-health/cancer (accessed August 14, 2024).
NIH. n.d.-b. NIH Grants Policy Statement: 4.1.14 Human Fetal Tissue Research. https://grants.nih.gov/grants/policy/nihgps/html5/section_4/4.1.14_human_fetal_tissue_research.htm (accessed August 21, 2024).
NIH. n.d.-c. NIH Grants Policy Statement: 4.2.7 Restriction on Abortion Funding. https://grants.nih.gov/grants/policy/nihgps/HTML5/section_4/4.2.7_restriction_on_abortion_funding.htm (accessed August 21, 2024).
NIH. 2013. Understanding Breast Cancer: Early Detection, Improved Treatments Save Lives. https://newsinhealth.nih.gov/sites/newsinhealth/files/2013/October/NIHNiHOct2013.pdf (accessed August 14, 2024).
Nordin, M. L., A. K. Azemi, A. H. Nordin, W. Nabgan, P. Y. Ng, K. Yusoff, N. Abu, K. P. Lim, Z. A. Zakaria, N. Ismail, and F. Azmi. 2023. Peptide-based vaccine against breast cancer: Recent advances and prospects. Pharmaceuticals 16(7).
Norton, M. C., K. R. Smith, T. Østbye, J. T. Tschanz, C. Corcoran, S. Schwartz, K. W. Piercy, P. V. Rabins, D. C. Steffens, I. Skoog, J. C. Breitner, and K. A. Welsh-Bohmer. 2010. Greater risk of dementia when spouse has dementia? The Cache County study. Journal of the American Geriatric Society 58(5):895–900.
O’Kelly, A. C., E. D. Michos, C. L. Shufelt, J. V. Vermunt, M. B. Minissian, O. Quesada, G. N. Smith, J. W. Rich-Edwards, V. D. Garovic, S. R. El Khoudary, and M. C. Honigberg. 2022. Pregnancy and reproductive risk factors for cardiovascular disease in women. Circulation Research 130(4):652–672.
Orgera, K., and A. Grover. 2024. States with Abortion Bans See Continued Decrease in U.S. MD Senior Residency Applicants. https://www.aamcresearchinstitute.org/our-work/data-snapshot/post-dobbs-2024 (accessed August 19, 2024).
Ossenkoppele, R., C. H. Lyoo, J. Jester-Broms, C. H. Sudre, H. Cho, Y. H. Ryu, J. Y. Choi, R. Smith, O. Strandberg, S. Palmqvist, J. Kramer, A. L. Boxer, M. L. Gorno-Tempini, B. L. Miller, R. La Joie, G. D. Rabinovici, and O. Hansson. 2020. Assessment of demographic, genetic, and imaging variables associated with brain resilience and cognitive resilience to pathological tau in patients with Alzheimer disease. JAMA Neurology 77(5):632–642.
Palatnik, A., R. K. Harrison, R. J. Walker, M. Y. Thakkar, and L. E. Egede. 2022. Maternal racial and ethnic disparities in glycemic threshold for pharmacotherapy initiation for gestational diabetes. Journal of Maternal-Fetal & Neonatal Medicine 35(1):58–65.
Pallerla, S., A. Abdul, J. Comeau, and S. Jois. 2021. Cancer vaccines, treatment of the future: With emphasis on HER2-positive breast cancer. International Journal of Molecular Sciences 22(2).
Parikh, N. I., J. M. Gonzalez, C. A. M. Anderson, S. E. Judd, K. M. Rexrode, M. A. Hlatky, E. P. Gunderson, J. J. Stuart, and D. Vaidya, on behalf of the American Heart Association Council on Epidemiology and Prevention; Council on Arteriosclerosis, Thrombosis, and Vascular Biology; Council on Cardiovascular and Stroke Nursing; and the Stroke
Council. 2021. Adverse pregnancy outcomes and cardiovascular disease risk: Unique opportunities for cardiovascular disease prevention in women: A scientific statement from the American Heart Association. Circulation 143(18):e902–e916.
Patterson, R., I. Balan, A. L. Morrow, and S. Meltzer-Brody. 2024. Novel neurosteroid therapeutics for post-partum depression: Perspectives on clinical trials, program development, active research, and future directions. Neuropsychopharmacology 49(1):67–72.
Payne, J. L., and J. Maguire. 2019. Pathophysiological mechanisms implicated in postpartum depression. Frontiers in Neuroendocrinology 52:165–180.
Peacock, K., K. Carlson, and K. M. Ketvertis. 2023. Menopause. In Statpearls. Treasure Island, FL: StatPearls Publishing.
Petersen, E. E., N. L. Davis, D. Goodman, S. Cox, C. Syverson, K. Seed, C. Shapiro-Mendoza, W. M. Callaghan, and W. Barfield. 2019. Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. MMWR 68(35):762–765.
Phimphasone-Brady, P., C. E. Page, D. A. Ali, H. C. Haller, and K. A. Duffy. 2023. Racial and ethnic disparities in women’s mental health: A narrative synthesis of systematic reviews and meta-analyses of the U.S.-based samples. Fertility and Sterility 119(3):364–374.
Pinna, G. 2020. Allopregnanolone, the neuromodulator turned therapeutic agent: Thank you, next? Frontiers in Endocrinology 11:236.
Practice Committee of the American Society for Reproductive Medicine. 2012. Evaluation and treatment of recurrent pregnancy loss: A committee opinion. Fertility and Sterility 98(5):1103–1111.
Practice Committee of the American Society for Reproductive Medicine. 2013. Definitions of infertility and recurrent pregnancy loss: A committee opinion. Fertility and Sterility 99(1):63.
Quenby, S., I. D. Gallos, R. K. Dhillon-Smith, M. Podesek, M. D. Stephenson, J. Fisher, J. J. Brosens, J. Brewin, R. Ramhorst, E. S. Lucas, R. C. McCoy, R. Anderson, S. Daher, L. Regan, M. Al-Memar, T. Bourne, D. A. MacIntyre, R. Rai, O. B. Christiansen, M. Sugiura-Ogasawara, J. Odendaal, A. J. Devall, P. R. Bennett, S. Petrou, and A. Coomarasamy. 2021. Miscarriage matters: The epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet 397(10285):1658–1667.
Raglan, G. B., S. M. Lannon, K. M. Jones, and J. Schulkin. 2016. Racial and ethnic disparities in preterm birth among American Indian and Alaska Native women. Maternal and Child Health Journal 20(1):16–24.
Ralph, L. J., E. B. Schwarz, D. Grossman, and D. G. Foster. 2019. Self-reported physical health of women who did and did not terminate pregnancy after seeking abortion services. Annals of Internal Medicine 171(4):238–247.
Rassie, K., R. Giri, A. E. Joham, H. Teede, and A. Mousa. 2022. Human placental lactogen in relation to maternal metabolic health and fetal outcomes: A systematic review and meta-analysis. International Journal of Molecular Sciences 23(24).
Reddy, D. S., R. H. Mbilinyi, and E. Estes. 2023. Preclinical and clinical pharmacology of brexanolone (allopregnanolone) for postpartum depression: A landmark journey from concept to clinic in neurosteroid replacement therapy. Psychopharmacology 240(9): 1841–1863.
Reekes, T. H., C. I. Higginson, C. R. Ledbetter, N. Sathivadivel, R. M. Zweig, and E. A. Disbrow. 2020. Sex specific cognitive differences in parkinson disease. NPJ Parkinson’s Disease 6(1):7.
Regan, L., R. Rai, S. Saravelos, and T.-C. Li on behalf of the Royal College of Obstetricians and Gynaecologists. 2023. Recurrent miscarriage: Green-top guideline no. 17. BJOG 130(12):e9–e39.
Reis, F. M., E. Bloise, and T. M. Ortiga-Carvalho. 2016. Hormones and pathogenesis of uterine fibroids. Best Practice and Research Clinical Obstetrics and Gynaecology 34:13–24.
Rimel, B. J., C. A. Kunos, N. Macioce, and S. M. Temkin. 2022. Current gaps and opportunities in screening, prevention, and treatment of cervical cancer. Cancer 128(23):4063–4073.
Ritchie, K., C. W. Ritchie, K. Yaffe, I. Skoog, and N. Scarmeas. 2015. Is late-onset Alzheimer’s disease really a disease of midlife? Alzheimer’s & Dementia 1(2):122–130.
Rome, D., A. Sales, R. Leeds, J. Usseglio, T. Cornelius, C. Monk, K. G. Smolderen, and N. Moise. 2022. A narrative review of the association between depression and heart disease among women: Prevalence, mechanisms of action, and treatment. Current Atherosclerosis Reports 24(9):709–720.
Rossen, L. M., B. E. Hamilton, J. C. Abma, E. C. W. Gregory, V. Beresovsky, A. V. Resendez, A. Chandra, and J. A. Martin. 2023. Updated methodology to estimate overall and unintended pregnancy rates in the United States: Data evaluation and methods research. Hyattsville, MD: National Center for Health Statistics, Centers for Disease Control and Prevention.
Rössler, W., V. Ajdacic-Gross, A. Riecher-Rössler, J. Angst, and M. P. Hengartner. 2016. Does menopausal transition really influence mental health? Findings from the prospective long-term Zurich study. World Psychiatry 15(2):146–154.
Rumble, M. E., P. Okoyeh, and R. M. Benca. 2023. Sleep and women’s mental health. Psychiatric Clinics of North America 46(3):527–537.
Salomon, J. A., T. Vos, D. R. Hogan, M. Gagnon, M. Naghavi, A. Mokdad, N. Begum, R. Shah, M. Karyana, S. Kosen, M. R. Farje, G. Moncada, A. Dutta, S. Sazawal, A. Dyer, J. Seiler, V. Aboyans, L. Baker, A. Baxter, E. J. Benjamin, K. Bhalla, A. Bin Abdulhak, F. Blyth, R. Bourne, T. Braithwaite, P. Brooks, T. S. Brugha, C. Bryan-Hancock, R. Buchbinder, P. Burney, B. Calabria, H. Chen, S. S. Chugh, R. Cooley, M. H. Criqui, M. Cross, K. C. Dabhadkar, N. Dahodwala, A. Davis, L. Degenhardt, C. Díaz-Torné, E. R. Dorsey, T. Driscoll, K. Edmond, A. Elbaz, M. Ezzati, V. Feigin, C. P. Ferri, A. D. Flaxman, L. Flood, M. Fransen, K. Fuse, B. J. Gabbe, R. F. Gillum, J. Haagsma, J. E. Harrison, R. Havmoeller, R. J. Hay, A. Hel-Baqui, H. W. Hoek, H. Hoffman, E. Hogeland, D. Hoy, D. Jarvis, G. Karthikeyan, L. M. Knowlton, T. Lathlean, J. L. Leasher, S. S. Lim, S. E. Lipshultz, A. D. Lopez, R. Lozano, R. Lyons, R. Malekzadeh, W. Marcenes, L. March, D. J. Margolis, N. McGill, J. McGrath, G. A. Mensah, A. C. Meyer, C. Michaud, A. Moran, R. Mori, M. E. Murdoch, L. Naldi, C. R. Newton, R. Norman, S. B. Omer, R. Osborne, N. Pearce, F. Perez-Ruiz, N. Perico, K. Pesudovs, D. Phillips, F. Pourmalek, M. Prince, J. T. Rehm, G. Remuzzi, K. Richardson, R. Room, S. Saha, U. Sampson, L. Sanchez-Riera, M. Segui-Gomez, S. Shahraz, K. Shibuya, D. Singh, K. Sliwa, E. Smith, I. Soerjomataram, T. Steiner, W. A. Stolk, L. J. Stovner, C. Sudfeld, H. R. Taylor, I. M. Tleyjeh, M. J. van der Werf, W. L. Watson, D. J. Weatherall, R. Weintraub, M. G. Weisskopf, H. Whiteford, J. D. Wilkinson, A. D. Woolf, Z. J. Zheng, C. J. Murray, and J. B. Jonas. 2012. Common values in assessing health outcomes from disease and injury: Disability weights measurement study for the Global Burden of Disease study 2010. Lancet 380(9859):2129–2143.
Salomon, J. A., J. A. Haagsma, A. Davis, C. M. de Noordhout, S. Polinder, A. H. Havelaar, A. Cassini, B. Devleesschauwer, M. Kretzschmar, N. Speybroeck, C. J. L. Murray, and T. Vos. 2015. Disability weights for the Global Burden of Disease 2013 study. Lancet Global Health 3(11):e712–e723.
Santen, R. J., H. Brodie, E. R. Simpson, P. K. Siiteri, and A. Brodie. 2009. History of aromatase: Saga of an important biological mediator and therapeutic target. Endocrine Reviews 30(4):343–375.
Sassi, F. 2006. Calculating QALYs, comparing QALY and DALY calculations. Health Policy Plan 21(5):402–408.
Sateia, M. J. 2014. International classification of sleep disorders-third edition. Chest 146(5):1387–1394.
Sayres Van Niel, M., and J. L. Payne. 2020. Perinatal depression: A review. Cleveland Clinic Journal of Medicine 87(5):273–277.
Scalici, J., M. A. Finan, J. Black, M. D. Harmon, W. Nicolson, H. A. Lankes, W. E. Brady, and R. P. Rocconi. 2015. Minority participation in gynecologic oncology group (GOG) studies. Gynecologic Oncology 138(2):441–444.
Schmidt, P. J., N. Haq, and D. R. Rubinow. 2004. A longitudinal evaluation of the relationship between reproductive status and mood in perimenopausal women. American Journal of Psychiatry 161(12):2238–2244.
Schoenbaum, M., J. M. Sutherland, A. Chappel, S. Azrin, A. B. Goldstein, A. Rupp, and R. K. Heinssen. 2017. Twelve-month health care use and mortality in commercially insured young people with incident psychosis in the United States. Schizophrenia Bulletin 43(6):1262–1272.
Schott, S. L., A. Adams, R. J. Dougherty, T. Montgomery, F. C. Lapite, and F. E. Fletcher. 2023. Renewed calls for abortion-related research in the post-Roe era. Frontiers Public Health 11:1322299.
Sefah, N., S. Ndebele, L. Prince, E. Korasare, M. Agbleke, A. Nkansah, H. Thompson, A. Al-Hendy, and A. A. Agbleke. 2022. Uterine fibroids—causes, impact, treatment, and lens to the African perspective. Frontiers in Pharmacology 13:1045783.
Segal, N. A., J. M. Nilges, and W. M. Oo. 2024. Sex differences in osteoarthritis prevalence, pain perception, physical function and therapeutics. Osteoarthritis Cartilage 32(9):1045–1053.
Seritan, A. L., A.-M. Iosif, J. H. Park, D. DeatherageHand, R. L. Sweet, and E. B. Gold. 2010. Self-reported anxiety, depressive, and vasomotor symptoms: A study of perimenopausal women presenting to a specialized midlife assessment center. Menopause 17(2):410–415.
Shah, N. S., D. M. Lloyd-Jones, N. R. Kandula, M. D. Huffman, S. Capewell, M. O’Flaherty, K. N. Kershaw, M. R. Carnethon, and S. S. Khan. 2020. Adverse trends in premature cardiometabolic mortality in the United States, 1999 to 2018. Journal of the American Heart Association 9(23):e018213.
Shah, N. S., M. C. Wang, P. M. Freaney, A. M. Perak, M. R. Carnethon, N. R. Kandula, E. P. Gunderson, K. M. Bullard, W. A. Grobman, M. J. O’Brien, and S. S. Khan. 2021. Trends in gestational diabetes at first live birth by race and ethnicity in the U.S., 2011–2019. JAMA 326(7):660–669.
Shaw, C., E. Hayes-Larson, M. M. Glymour, C. Dufouil, T. J. Hohman, R. A. Whitmer, L. C. Kobayashi, R. Brookmeyer, and E. R. Mayeda. 2021. Evaluation of selective survival and sex/gender differences in dementia incidence using a simulation model. JAMA Network Open 4(3):e211001.
Shi, Y., D. Tan, B. Hao, X. Zhang, W. Geng, Y. Wang, J. Sun, and Y. Zhao. 2022. Efficacy of intravenous immunoglobulin in the treatment of recurrent spontaneous abortion: A systematic review and meta-analysis. American Journal of Reproductive Immunology 88(5):e13615.
Siegel, R. L., A. N. Giaquinto, and A. Jemal. 2024. Cancer statistics, 2024. CA 74(1):12–49.
Silverwood, V., M. Blagojevic-Bucknall, C. Jinks, J. L. Jordan, J. Protheroe, and K. P. Jordan. 2015. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthritis and Cartilage 23(4):507–515.
Slaughter-Acey, J., K. Behrens, A. Claussen, T. Usset, C. Neerland, S. Bilal-Roby, H. Bashir, A. Westby, B. Wagner, M. Dixon, M. Xiao, and M. Butler. 2023. Social and structural determinants of maternal morbidity and mortality: An evidence map. Rockville, MD: Agency for Healthcare Research and Quality.
Spencer, R. J., L. W. Rice, C. Ye, K. Woo, and S. Uppal. 2019. Disparities in the allocation of research funding to gynecologic cancers by funding to lethality scores. Gynecologic Oncology 152(1):106–111.
Srikanth, V. K., J. L. Fryer, G. Zhai, T. M. Winzenberg, D. Hosmer, and G. Jones. 2005. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis and Cartilage 13(9):769–781.
St. Pierre, A., J. Zaharatos, D. Goodman, and W. M. Callaghan. 2018. Challenges and opportunities in identifying, reviewing, and preventing maternal deaths. Obstetrics and Gynecology 131(1):138–142.
Staff, A. C. 2019. The two-stage placental model of preeclampsia: An update. Journal of Reproductive Immunology 134–135:1–10.
Statista. 2023. Resident Population of the United States by Sex and Age as of July 1, 2022. https://www.statista.com/statistics/241488/population-of-the-us-by-sex-and-age/ (accessed 7/12/2024, 2024).
Stevenson, A. J., and L. Root. 2024. Trends in maternal death post-Dobbs v Jackson Women’s Health. JAMA Network Open 7(8):e2430035.
Stewart, S. L., N. Lakhani, P. M. Brown, O. A. Larkin, A. R. Moore, and N. S. Hayes. 2013. Gynecologic cancer prevention and control in the National Comprehensive Cancer Control Program: Progress, current activities, and future directions. Jounal of Women’s Health 22(8):651–657.
Sundermann, E. E., P. M. Maki, L. H. Rubin, R. B. Lipton, S. Landau, and A. Biegon. 2016. Female advantage in verbal memory: Evidence of sex-specific cognitive reserve. Neurology 87(18):1916–1924.
Sundermann, E. E., M. S. Panizzon, X. Chen, M. Andrews, D. Galasko, and S. J. Banks, for the Alzheimer’s Disease Neuroimaging Initiative. 2020. Sex differences in Alzheimer’s-related Tau biomarkers and a mediating effect of testosterone. Biology of Sex Differences 11(1):33.
Surana, K. 2024a. Abortion Bans Have Delayed Emergency Medical Care. In Georgia, Experts Say This Mother’s Death Was Preventable. https://www.propublica.org/article/georgia-abortion-ban-amber-thurman-death (accessed October 10, 2024).
Surana, K. 2024b. Afraid to Seek Care Amid Georgia’s Abortion Ban, She Stayed Home and Died. https://www.propublica.org/article/candi-miller-abortion-ban-death-georgia (accessed October 10, 2024).
Sweeting, A., W. Hannah, H. Backman, P. Catalano, M. Feghali, W. H. Herman, M.-F. Hivert, J. Immanuel, C. Meek, M. L. Oppermann, C. J. Nolan, U. Ram, M. I. Schmidt, D. Simmons, T. Chivese, and K. Benhalima. 2024. Epidemiology and management of gestational diabetes. Lancet 404(10448):175–192.
Swenson, C. 2024. Research on Pelvic Floor Disorders. https://www.nationalacademies.org/documents/embed/link/LF2255DA3DD1C41C0A42D3BEF0989ACAECE3053A6A9B/file/DDCEB46107AB492040A1FCD09695BB1812A6FF641CBB?noSaveAs=1 (accessed July 18, 2024).
Szilagyi, I. A., J. H. Waarsing, J. B. J. van Meurs, S. M. A. Bierma-Zeinstra, and D. Schiphof. 2023. A systematic review of the sex differences in risk factors for knee osteoarthritis. Rheumatology 62(6):2037–2047.
Taiwo, T. K., K. Goode, P. M. Niles, K. Stoll, N. Malhotra, and S. Vedam. 2024. Perinatal mood and anxiety disorder and reproductive justice: Examining unmet needs for mental health and social services in a national cohort. Health Equity 8(1):3–13.
Terlizzi, E. P., and M. A. Villarroel. 2020. Symptoms of generalized anxiety disorder among adults: United States, 2019. NCHS Data Brief (378):1–8.
Tillmanns, T., A. Masri, C. Stewart, D. Chase, A. Karnezis, L.-m. Chen, and R. Urban. 2024. Advanced endometrial cancer—the next generation of treatment: A Society of Gynecologic Oncology Journal Club clinical commentary. Gynecologic Oncology Reports 55:101462.
Tipton, P., N. Bülbül, J. Crook, Z. Quicksall, O. Ross, R. Uitti, Z. Wszolek, and N. Ertekin-Taner. 2021. Effects of sex and APOE on Parkinson’s disease-related cognitive decline. Neurologia i Neurochirurgia Polska 55(6):559–566.
Towner, M., J. J. Kim, M. A. Simon, D. Matei, and D. Roque. 2022. Disparities in gynecologic cancer incidence, treatment, and survival: A narrative review of outcomes among Black and White women in the United States. International Journal of Gynecological Cancer 32(7):931–938.
Trost, S., J. Beauregard, G. Chandra, F. Njie, J. Berry, A. Harvey, and D. A. Goodman. 2022. Pregnancy-related deaths: Data from maternal mortality review committees in 36 U.S. states, 2017–2019. Atlanta, GA: Centers for Disease Control and Prevention.
Tsao, C. W., A. W. Aday, Z. I. Almarzooq, C. A. M. Anderson, P. Arora, C. L. Avery, C. M. Baker-Smith, A. Z. Beaton, A. K. Boehme, A. E. Buxton, Y. Commodore-Mensah, M. S. V. Elkind, K. R. Evenson, C. Eze-Nliam, S. Fugar, G. Generoso, D. G. Heard, S. Hiremath, J. E. Ho, R. Kalani, D. S. Kazi, D. Ko, D. A. Levine, J. Liu, J. Ma, J. W. Magnani, E. D. Michos, M. E. Mussolino, S. D. Navaneethan, N. I. Parikh, R. Poudel, M. Rezk-Hanna, G. A. Roth, N. S. Shah, M. P. St-Onge, E. L. Thacker, S. S. Virani, J. H. Voeks, N. Y. Wang, N. D. Wong, S. S. Wong, K. Yaffe, and S. S. Martin. 2023. Heart disease and stroke statistics—2023 update: A report from the American Heart Association. Circulation 147(8):e93–e621.
U.K. Health Security Agency. 2015. GBD Compare: A New Data Tool for Professionals. https://ukhsa.blog.gov.uk/2015/09/15/gbd-compare-a-new-data-tool-for-professionals/ (accessed August 13, 2024).
Ulm, M., A. V. Ramesh, K. M. McNamara, S. Ponnusamy, H. Sasano, and R. Narayanan. 2019. Therapeutic advances in hormone-dependent cancers: Focus on prostate, breast and ovarian cancers. Endocrine Connections 8(2):R10–R26.
USPSTF (U.S. Preventive Services Task Force). 2024. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. JAMA 331(22):1918–1930.
van den Akker, T., M. Nair, M. Goedhart, J. Schutte, T. Schaap, and M. Knight. 2017. Maternal mortality: Direct or indirect has become irrelevant. Lancet Global Health 5(12):e1181.
Vigo, D., L. Jones, R. Atun, and G. Thornicroft. 2022. The true global disease burden of mental illness: Still elusive. Lancet Psychiatry 9(2):98–100.
Vilda, D., M. E. Wallace, C. Daniel, M. G. Evans, C. Stoecker, and K. P. Theall. 2021. State abortion policies and maternal death in the United States, 2015–2018. American Journal of Public Health 111(9):1696–1704.
Vitaliano, P. P. 2010. An ironic tragedy: Are spouses of persons with dementia at higher risk for dementia than spouses of persons without dementia? Journal of the American Geriatrics Society 58(5):976–978.
Vogel, B., M. Acevedo, Y. Appelman, C. N. Bairey Merz, A. Chieffo, G. A. Figtree, M. Guerrero, V. Kunadian, C. S. P. Lam, A. Maas, A. S. Mihailidou, A. Olszanecka, J. E. Poole, C. Saldarriaga, J. Saw, L. Zühlke, and R. Mehran. 2021. The Lancet Women and Cardiovascular Disease Commission: Reducing the global burden by 2030. Lancet 397(10292):2385–2438.
Wariso, B. A., G. M. Guerrieri, K. Thompson, D. E. Koziol, N. Haq, P. E. Martinez, D. R. Rubinow, and P. J. Schmidt. 2017. Depression during the menopause transition: Impact on quality of life, social adjustment, and disability. Archive of Women’s Mental Health 20(2):273–282.
Weiner, S. 2022. How the Repeal of Roe v. Wade Will Affect Training in Abortion and Reproductive Health. https://www.aamc.org/news/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health (accessed August 15, 2024).
Whetstone, S., W. Burke, S. S. Sheth, R. Brooks, A. Cavens, K. Huber-Keener, D. M. Scott, B. Worly, and D. Chelmow. 2022. Health disparities in uterine cancer: Report from the Uterine Cancer Evidence Review Conference. Obstetrics & Gynecology 139(4):645–659.
Whiteley, J., M. DiBonaventura, J. S. Wagner, J. Alvir, and S. Shah. 2013. The impact of menopausal symptoms on quality of life, productivity, and economic outcomes. Journal of Women’s Health 22(11):983–990.
WHO (World Health Organization). n.d. Maternal Deaths. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/ (accessed August 14, 2024).
Wolfova, K., Z. Csajbok, A. Kagstrom, I. Kåreholt, and P. Cermakova. 2021. Role of sex in the association between childhood socioeconomic position and cognitive ageing in later life. Scientific Reports 11(1):4647.
Woods, N. F., and E. S. Mitchell. 2005. Symptoms during the perimenopause: Prevalence, severity, trajectory, and significance in women’s lives. American Journal of Medicine 118(12, Suppl 2):14–24.
Wu, P., M. Gulati, C. S. Kwok, C. W. Wong, A. Narain, S. O’Brien, C. A. Chew-Graham, G. Verma, U. T. Kadam, and M. A. Mamas. 2018. Preterm delivery and future risk of maternal cardiovascular disease: A systematic review and meta-analysis. Journal of the American Heart Association 7(2).
Yaffe, K., A. M. Laffan, S. L. Harrison, S. Redline, A. P. Spira, K. E. Ensrud, S. Ancoli-Israel, and K. L. Stone. 2011. Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. JAMA 306(6):613–619.
Yamada, H., M. Deguchi, S. Saito, T. Takeshita, M. Mitsui, T. Saito, T. Nagamatsu, K. Takakuwa, M. Nakatsuka, S. Yoneda, K. Egashira, M. Tachibana, K. Matsubara, R. Honda, A. Fukui, K. Tanaka, K. Sengoku, T. Endo, and H. Yata. 2022. Intravenous immunoglobulin treatment in women with four or more recurrent pregnancy losses: A double-blind, randomised, placebo-controlled trial. eClinicalMedicine 50.
Ye, W., C. Luo, J. Huang, C. Li, Z. Liu, and F. Liu. 2022. Gestational diabetes mellitus and adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 377:e067946.
Young, S. 2024. Endometriosis Research: Barriers to Progress. Presentation to the NASEM Committee on the Assessment of NIH Research on Women’s Health, Meeting 2 (March 7, 2024). https://www.nationalacademies.org/documents/embed/link/LF2255DA3DD1C41C0A42D3BEF0989ACAECE3053A6A9B/file/D88A63BB015C48DB61FD1575954A59AE902C6A858D9C?noSaveAs=1 (accessed August 14, 2024).
Zhang, C., C. Zhang, Q. Wang, Z. Li, J. Lin, and H. Wang. 2020a. Differences in stage of cancer at diagnosis, treatment, and survival by race and ethnicity among leading cancer types. JAMA Network Open 3(4):e202950.
Zhang, M., P. Wan, K. Ng, K. Singh, T. H. Cheng, I. Velickovic, M. Dalloul, and D. Wlody. 2020b. Preeclampsia among African American pregnant women: An update on prevalence, complications, etiology, and biomarkers. Obstetrical & Gynecological Survey 75(2):111–120.
This page intentionally left blank.





































































