Prepregnancy BMI and Gestational Weight Gain: New Evidence, Emerging Innovations, and Policy Implications: Proceedings of a Workshop (2026)
Chapter: 3 Social Economic Predictors of Prepregnancy BMI and Gestational Weight Gain
3
Social and Economic Predictors of Prepregnancy BMI and Gestational Weight Gain
SOCIAL, ECONOMIC, AND POLICY PREDICTORS
Social and structural determinants, at both the individual and community levels, have a large effect on health, said Angela Odoms-Young, Cornell University. She explained that social determinants of health (SDOH) are the conditions where people are born, grow, live, work, and age. These conditions are shaped by broader forces and systems like economic policies and social norms. Structural determinants of health are the underlying systems and mechanisms—such as political structures, social policies, and economic systems—that create and maintain inequities in social determinants, which lead to unfair differences in health outcomes. SDOH play a crucial role in maternal, fetal, and newborn health, prepregnancy body mass index (BMI), and gestational weight gain (GWG), said Odoms-Young, and the pathways linking SDOH to perinatal outcomes are multifactorial and complex.
Because of inequities in SDOH, certain populations experience greater social disadvantage. Social disadvantage, Odoms-Young stated, refers to the barriers and forms of exclusion individuals encounter as a result of their membership in marginalized social groups, which limit access to opportunities and resources necessary for full participation in society. These disadvantages manifest across multiple domains, economic, environmental, and institutional, and have measurable effects on health and well-being (Avorgbedor et al., 2022; Kinsey et al., 2023). For instance, Black women are disproportionately likely to reside in socioeconomically disadvantaged neighborhoods, where structural conditions such as inadequate housing, limited access to healthy foods, and environmental hazards can negatively
influence health before and during pregnancy, contributing to adverse maternal and infant outcomes (Sharma et al., 2022). Social disadvantage is place-based, and maps of the United States demonstrate the correlation between social disadvantage and poor health outcomes. Counties with lower median household income are more highly concentrated in southern states, and people in these states are less likely to move upward in social class. These states are also the areas with higher levels of negative outcomes in maternal and child health, said Odoms-Young. There are a variety of ways to measure social disadvantage. It can be measured using an individual variable—such as income—or a composite index that combines multiple individual variables into a single summary score. Indexes are a way of capturing the synergistic effect of social conditions and the multiple pathways on which they have an effect. Some measures incorporate assessments of social class, such as occupation, educational attainment, or self-reported perceptions of social standing.
Several studies have looked at the association between social disadvantage and perinatal outcomes, said Odoms-Young. These studies used a variety of measurements, including:
- Neighborhood socioeconomic disadvantage (Mendez et al., 2014)
- Neighborhood structural racism (Avorgbedor et al., 2022)
- Neighborhood deprivation (e.g., crime, healthy food availability, unemployment; Headen et al., 2018; Kinsey et al., 2023; Sassin et al., 2025)
- Education, income, income-to-needs ratio, marital status (Nunnery et al., 2018; O’Brien et al., 2018).
Odoms-Young noted that while the literature is clear about the link between social disadvantage and the risk of negative perinatal outcomes, there is considerably less information about the pathways or mechanisms by which the relationship operates. A 2022 framework for social inequalities and perinatal outcomes described how socioeconomic and political context, along with individual socioeconomic characteristics, contribute to differences in intermediary SDOH such as living conditions, food availability, physical activity, nutrition, stress, and social support. These intermediary SDOH then affect mental and physical health, which affect perinatal outcomes (Figure 3-1; Simoncic et al., 2022). Understanding these pathways, the multiple causal factors, and the interactions among them, is critical for developing interventions that work, said Odoms-Young.
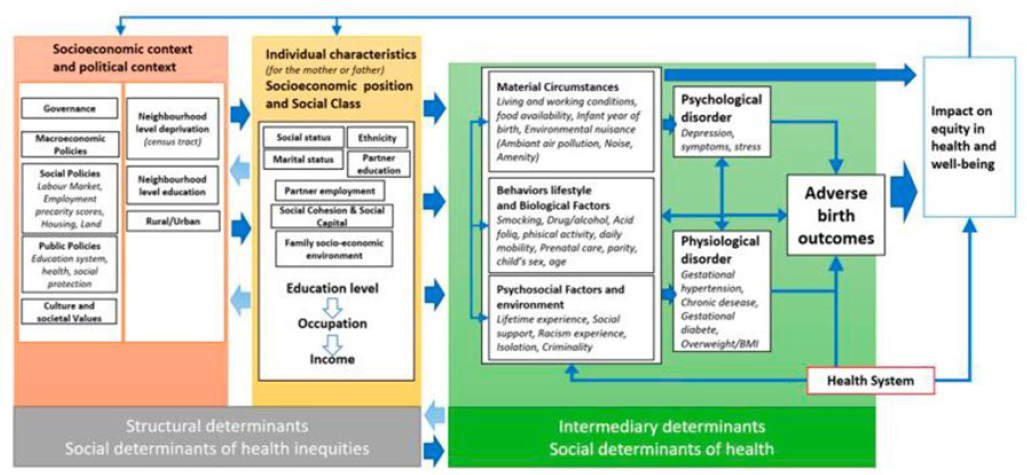
NOTE: BMI = body mass index.
SOURCE: Presented by Angela Odoms-Young on September 5, 2025; Simoncic et al., 2022. CC BY 4.0.
CONTRIBUTION OF HEALTH INEQUITIES
As Odoms-Young discussed, there are numerous structural drivers of health outcomes, said Stephanie Navarro Silvera, Montclair University. These include socioeconomic factors, the social environment, the physical environment, and access to health care. There are data that show that if improvements are made in these areas, there will be better health outcomes across the life course. Focusing specifically on structural contributors to perinatal health, she noted that Black and Hispanic women have higher rates of prepregnancy obesity, and she said that there is evidence to suggest that these disparities reflect systemic inequities across race, socioeconomic status, and geography. In particular, disparities in access to healthy food and the built environment may affect prepregnancy weight, GWG, and perinatal health outcomes.
Access to healthy food is a challenge in poorer neighborhoods, said Silvera. As neighborhood poverty increases, there is a decrease in supermarkets and an increase in convenience stores. This problem is worse in Black neighborhoods; at equal levels of poverty, Black census tracts have the fewest supermarkets and White tracts have the most. It has been estimated that around 31 percent of White people have a supermarket in their census tract of residence, compared to only 8 percent of Black people (Morland et al., 2002). Silvera noted that there is an association between limited food access and structural racism, specifically, issues related to redlining, gentrification, and racial segregation. This lack of access to healthy food makes a difference to health. Studies shows that people living in areas with limited access to healthy food are more likely to consume foods with poorer nutritional quality and are more likely to have obesity and metabolic disorders. One pregnancy-specific study found that living in food-insecure neighborhoods was associated with an increased likelihood of morbidity during pregnancy (Wood et al., 2023). Further, it found that the relationship between adiposity and socioeconomic status was mediated by food desert severity; that is, pregnant individuals with lower socioeconomic status are more likely to live in a food desert and thus more likely to be overweight.
The neighborhood in which a person lives also affects their access to park spaces, sidewalks, and other opportunities for physical activity, said Silvera. A 2008 study looked at access to recreational facilities and found that Black and Hispanic neighborhoods were significantly more likely than White neighborhoods to not have recreational facilities (Moore et al., 2008). In addition, almost 75 percent of low-income neighborhoods had no facilities, compared to 45 percent of high-income neighborhoods. Lack of facilities for physical activity matters to health, said Silvera. A cross-sectional study of 50,000 women found that living in greener neighborhoods
was associated with higher levels of activity and lower levels of obesity (Villeneuve et al., 2018).
There have been policy efforts to address these disparities, said Silvera. For example, in King County, Washington, an ordinance guarantees equal access to facilities and services across neighborhoods. There is a need for research on these types of policies to measure their effect and to examine how policy can drive better health. Silvera noted that with recent federal budget cuts to food security programs, there will unfortunately be many opportunities to study the effect of policy on pregnancy health outcomes. In addition to this research gap, there is a need for research on contributing factors that explain the relationship between socioeconomic status and perinatal health; this is critical for designing intervention strategies that will be effective. In addition, there is a need for studies that focus on the intersectionality among multiple identities and characteristics, and how these factors interact to affect health. Silvera closed with a quote, “Every system is perfectly designed to get the results it gets.” She encouraged stakeholders to think more carefully about how systems can be better designed to get better results.
MATERNAL AND INFANT HEALTH IN THE MARSHALLESE COMMUNITY
Britni Ayers, University of Arkansas for Medical Sciences (UAMS), told workshop participants about her experiences working with the Marshallese community in Arkansas for the past 10 years as a maternal health researcher. Before this, Ayers home birthed and breastfed her own children, became a lactation consultant and midwife’s apprentice, and earned a Ph.D. in public policy with a focus on birth and breastfeeding policy. Ayers began by describing the background of the Marshallese. They come from a small group of islands in the South Pacific where the U.S. military tested nuclear weapons from 1946 to 1958. This testing—equivalent to 7,000 times that of Hiroshima—resulted in significant radiation fallout that killed off much of the fish and vegetation that the Marshallese relied on for food. The U.S. government began to provide “pantry foods” such as white rice and canned meats, and they conducted research on the Marshallese without consent. These experiences led to historical trauma and a deep distrust of researchers, said Ayers. There are about 16,000 Marshallese living in Arkansas; she explained that some Marshallese initially came to work in factories and the community followed owing to their collectivist culture.
In 2012, UAMS began a community-engaged research program with the local Marshallese. Community-engaged research, she explained, emphasizes identifying and focusing on the needs of the community; the Marshallese identified maternal health as a key priority. Pacific Islanders who reside
in the United States have poor perinatal outcomes, said Ayers, including preterm birth, low birth weight, preeclampsia, cesarean delivery, excessive GWG, and gestational diabetes. In a review of birth record data from the Arkansas Marshallese community specifically, 19 percent of infants were preterm, 15 percent were low birth weight, 15 percent received no prenatal care, and 50 percent did not attend all recommended prenatal care visits. Ayers said that her qualitative research with Marshallese women revealed a number of barriers to prenatal care, including transportation, health insurance, language barriers, and a sense of discrimination and feeling unwelcome in health care communities.
To address these barriers, Ayers created a program specifically for Marshallese women, adapting an existing model called Centering Pregnancy. Centering Pregnancy is a group prenatal program in which women come together for their prenatal care for 10 visits; the model has been demonstrated to reduce preterm birth and low birth weight, improve breastfeeding initiation and duration, and reduce excessive GWG. A Marshallese bilingual nurse led the program in the Marshallese language, said Ayers, and women felt comfortable asking their questions and talking about their culture. The sessions were catered with Marshallese food, which provided an opportunity to talk about portion control and appropriate GWG. With the program now in its 5th year, Ayers said she is excited to begin to analyze the data.
Another challenge in the Marshallese community is postpartum care, said Ayers. There is little postpartum support in Arkansas in general; it is the only state in which Medicaid does not cover postpartum care beyond the first 60 days. Ayers chose to create a postpartum program for the Marshallese that focused on breastfeeding and obesity. A 2016 study found that 90 percent of Marshallese adults in Arkansas were overweight or obese, and exclusive breastfeeding rates are very low. Exclusive breastfeeding for at least 6 months reduces the odds of obesity for the mother by 30 percent, explained Ayers, and the protective effects of breastfeeding increase with duration. Qualitative research found that women were not breastfeeding because of a lack of policy support, working outside the home, and feeling out of place breastfeeding in public. The mothers also tended to introduce solid foods early, with an emphasis on high starch and sugar foods such as white rice and sweetened condensed milk.
Ayers introduced a program called Centering Parenting, which is based on the same model as Centering Pregnancy; women attend nine sessions between 6 weeks and 12 months postpartum. Ayers noted that for the program to be successful, it needed to be culturally adapted to be appropriate for the community. For the sessions focused on food and nutrition, she and her colleagues began by conducting dietary recall of postpartum women to characterize the diet patterns and practices in the community.
The initial data from the dietary study, said Ayers, found that there was a high intake of seafood, white rice, sweet drinks, and added sugar and salt, and low intake of fruit, vegetables, dairy, and whole grains. These dietary patterns are related to the historical trauma of the community, said Ayers, so it is critical to be mindful and thoughtful when talking about food in the intervention.
Ayers and her colleagues engaged with Marshallese stakeholders to discuss the dietary recall study and how the program might be adapted for the community. For example, Ayers suggested that people could replace half of their white rice with brown rice; she said the Marshallese stakeholders laughed at this idea and said that the Marshallese “won’t do it.” In the end, they decided to focus on controlling portion size of rice instead. The Centering Parenting program was adapted and translated into Marshallese and was overall very successful. Community-engaged research takes time and patience, said Ayers, but focusing on issues of concern to the community and making cultural adaptations are both critical components for implementing a successful intervention.
This page intentionally left blank.







