Identifying Midlife Social Exposures That Might Modify Risks of Cognitive Impairment Associated with Early Life Disadvantage: Proceedings of a Workshop (2025)
Chapter: 6 Social Support and Integration (Neighborhoods)
6
Social Support and Integration (Neighborhoods)
NEIGHBORHOODS, COGNITIVE HEALTH, AND DEMENTIA RISK: CONCEPTS, CHALLENGES, AND DIRECTIONS
Michael Esposito, Assistant Professor of Sociology at the University of Minnesota, started by describing the unequal distribution of health outcomes across neighborhoods. Nearly 75 percent of place-based variation in mortality is attributable to census tracts (Boing et al., 2020). Looking at the extremes, there are nearly-20-year longevity gaps between communities in different parts of the country. Based on these data, one might simulate differences in cognitive outcomes, as shown in Figure 6-1. The horizontal range of the entire green distribution reflects the variation in predicted cognitive function that would appear if the same person were moved across a range of neighborhoods at the same point in time. The distance between the gray dashed line and the center point of the distribution summarizes the change in cognitive function an older adult is predicted to experience after aging five years. Thus, it is very common to observe neighborhood effects that outpace the impact of even multiple years of aging.
However, while the extent of variation is measurable, the reasons for the variation are less clear. Typical approaches are to look at concepts such as the percentage of residents living below the poverty line, the percentage of residents who identify as Black people, or other aggregations. This is more of a catalog of who is vulnerable to dementia risk than identification of what place-based factors are generating these inequalities. It results in a largely circular explanation, as stated by Cohen et al. in a forthcoming paper: communities are vulnerable to poor health because the residents
![A line graph or bell curve simulating how cognitive outcomes vary across census tracts. The line graph peaks at 0 with even ebbing to both -6 & 6. The y axis labeled destiny represents the number of census tracts. The x axis represents shift in cognitive function [centered on population-mean] which increases from -8 to 8 in increments of 4. A vertical dashed line at -1 represents the change in cognitive function an older adult is predicted to experience after aging 5 years. There is much more variation across census tracts in cognitive outcomes than appears even after aging 5 years.](https://uwnxt.nationalacademies.org/read/28909/assets/images/img-58-1.jpg)
SOURCE: Presentation by Michael Esposito on August 30, 2024.
possess the traits of vulnerability. Such explanations do not offer much insight into the causal processes leading to these differential vulnerabilities in the first place.
Esposito views the neighborhoods-determinant literature as approaching a dynamic turning point. More researchers are shifting toward interrogating concrete causal agents rather than the people and places shaped by them. This change in priorities has been precipitated by truly novel data collection, which enables descriptions of the built-in features located in people’s communities that present hazards or help on a daily basis: the place-based laws and regulations that constrain or facilitate the way people would like to live their lives, and even relational hazards like place-based exploitation that people are subjected to based on where they live (Graetz & Esposito, 2023; Purifoy & Seamster, 2021; Uhl et al., 2021). There still remains much room for theorizing and using new data to develop critical accounts of how neighborhoods produce cognitive inequalities.
Esposito cautioned that there are unavoidable conceptual challenges around what exposure means, particularly for neighborhood-based exposures that are experienced continuously over the entire life course. Given that people may move, and that neighborhoods themselves may change, a person’s life course may encompass exposures at a variety of levels. Esposito said researchers will need to rely on all sorts of inputs from
critical life course theories that indicate which treatment effects (of many) should be prioritized, along with boots-on-the-ground qualitative research to define exposures in ways that map how people really experience their neighborhoods.
NEIGHBORHOOD CONTEXTS ACROSS THE LIFESPAN AND MIDLIFE COGNITION
Elizabeth Muñoz, Assistant Professor of Human Development and Family Sciences, and Faculty Affiliate of the Center on Aging Population Sciences and the Population Research Center at the University of Texas at Austin, emphasized the importance of looking at midlife exposures. She noted that cognitive decline starts as early as age 20 and certainly by age 45, requiring us to start to map changes that manifest earlier in the lifespan (see Figure 6-2). She discussed neighborhood contexts as being social determinants of health: that is, the conditions in the environment where people are born and where they live, learn, work, play, worship, and age that affect a range of health outcomes. Neighborhoods have both structural and social aspects. Structural factors include neighborhood socioeconomic status, spatial components, and physical aspects of neighborhoods such as
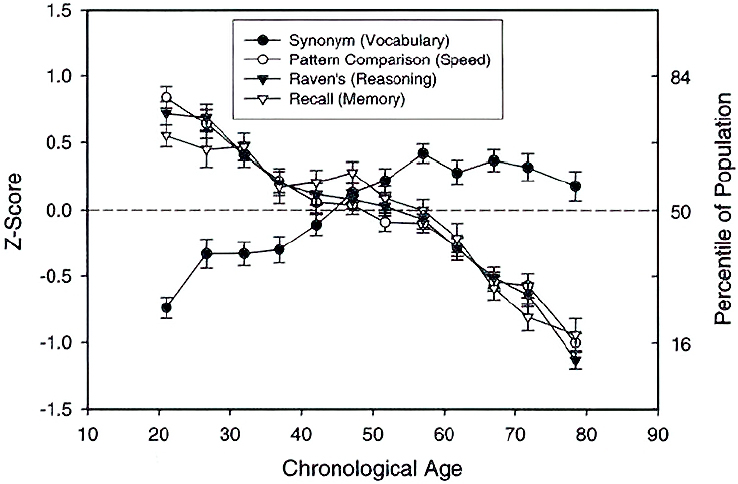
SOURCES: Presentation by Elizabeth Muñoz on August 30, 2024; based on Salthouse, 2009.
distance to parks and recreation and access to healthy foods. Social aspects include the social connections between neighbors and people’s sense of safety in a neighborhood. Structural and social factors can interact and influence one another.
Muñoz described a study of three cohorts of midlife adults or adults at the cusp of midlife who had similar measures of neighborhood context, using data from the Colorado Adoption/Twin Study of Lifespan Behavioral Development and Cognitive Aging (CATSLife) and the Effects of Stress on Cognitive Aging, Physiology and Emotion (ESCAPE) Study (Muñoz et al., 2020). Different neighborhood factors were associated with different types of cognitive decline. Lower levels of neighborhood safety were associated with lower executive and spatial functioning. Poor aesthetic quality and more neighborhood crime were both associated with lower spatial functioning. Lower social cohesion was associated with lower work and memory functioning. These associations were all above and beyond the following individual-level covariates: age, sex, race/ethnicity, education, marital status, employment status, financial strain, depressive symptoms, and self-reported health.
Taking a life course approach, Muñoz said one might think about how neighborhoods interact with timing within a lifespan. We know that early childhood is important for brain development. In young adulthood and midlife, the meaning of neighborhoods changes, with people moving out of their parents’ homes, starting their first full-time jobs, and settling into neighborhoods. In older adulthood and retirement, neighborhoods may increase in importance, with people spending more time in their neighborhoods. This may be a time when neighborhoods provide or take away resources that allow for cognitive maintenance.
Muñoz said the Leave-Behind Questionnaire of the HRS contains a neighborhood cohesion measure. Both the full neighborhood cohesion measure from the Leave-Behind Questionnaire scale and the individual item that matched the one neighborhood cohesion item from the Life History survey showed similar results (Choi et al., 2023). Early life neighborhood cohesion at age 10 and at the baseline assessment were both associated with higher levels of cognitive function, but there were no associations with rate of cognitive change.
Muñoz also described CATSLife.1 The project combines two studies of parents at midlife and measures early life childhood development, comprising 1,327 participants in the first assessment during 2015 through 2021. There are assessments yearly from birth through age 16 and then about every five years into early adulthood. New data were collected with NIA
___________________
1 https://www.colorado.edu/ibg/catslife/home; https://st1.niagads.org/portal/download-public/NG00145.v1/rn
funding between 2015 and 2021 when participants were as young as 28 (average age 33 years; range 28–51 years) and again six years later for CATSLife2 (the second wave of CATSLife). CATSLife has multiple cognitive assessments, identifying biomarkers (including of accelerated aging) and environmental factors, including longitudinal neighborhood change data. While the participants were born in Colorado, they are now scattered over the United States. CATSLife includes both lab-based cognitive assessments and ambulatory assessments using smartphone-based applications.
Another study described by Muñoz is the ESCAPE study, based on 256 individuals living in the Bronx, New York, between the ages of 25 and 65 and who were primarily non-Hispanic Black and Hispanic people (Muñoz et al., 2024). Participants were trained on using a smartphone to complete their cognitive assessments throughout their lives. The study found that greater neighborhood violence was associated with poor performance in the latent working memory construct, but it also found that this effect was primarily mediated or driven by the ambulatory, smartphone-based cognitive tasks, while there was no association using the lab-based cognitive tasks. This suggests that the modality of cognitive testing may be important.
Muñoz discussed a study she is currently involved in (Perceived Ethnic Discrimination and Cognitive Function in Mexican-origin Adults) focused on Latinx individuals between the ages of 45 and 65 in Austin, Texas. The study has a two-week period throughout which surveys are administered four times a day. It moves away from a fixed definition of neighborhood and captures more of the dynamic nature of neighborhood experiences.
Muñoz concluded that evaluating multiple domains of neighborhoods is important, as they may be differently linked with different cognitive abilities; there is a need to think about the structural and social components as well as the objective and self-reported assessments. Objective measures may represent something different from the self-report assessments, which may represent more of the lived experience of individuals. The timing of neighborhood experiences and exposure is important. There are independent effects of neighborhood cohesion in early life and in midlife. However, Muñoz said there is still a need to examine potentially distinct mechanisms of the effects from early life and concurrently in midlife or late midlife. For instance, it may be that early life exposures have a more sustained effect on levels of cognitive function compared to context in adulthood. Looking at the effects of neighborhood domains by timing as well may show that some domains are more or less influential in some time periods compared to others. Also, the modality of cognitive assessments may matter. It may be that measuring cognition in people’s everyday lives where they learn, work, play, and worship will give us a more nuanced and potentially more accurate understanding of the link between neighborhoods and cognitive function.
QUALITATIVE AND MIXED METHODS APPROACHES TO NEIGHBORHOODS AND COGNITIVE AGING
Jessica Finlay, Assistant Professor in the Department of Geography and Institute of Behavioral Science at the University of Colorado Boulder, spoke about some of the challenges facing health geographers. One is the Modifiable Areal Unit Problem, which posits that the spatial unit or geography at which we measure exposure matters and may change the outcomes of a study. How do we measure one consistent neighborhood boundary when all of us have different lived experiences influenced by a host of individual and contextual characteristics? Figure 6-3 shows some of the possibilities. A census tract is one tool that is standardized and readily available, averaging about 4,000 people. Another approach is to define a neighborhood using a one-mile buffer around a respondent’s home. A third is to ask respondents how many blocks they think of as their neighborhood (but note that they might not place themselves in the center of that neighborhood but rather place themselves on the edge).
A second problem described by Finlay is spatial polygamy. Exposures are not limited to just one time point or one home address location. Instead, people live and are exposed to multiple environments across the day and across time where they live, work, play, and pray. For example, there is an effort in the HRS to think about work environments as well as home environments.
To explore these issues, Finlay described her work with Esposito, conducting 60 qualitative interviews in the Minneapolis/St. Paul metropolitan area through a purposeful sample of understudied populations who were

SOURCE: Presented to the panel by Jessica Finlay on August 30, 2024.
stratified by age groups, ranging from 18 to 80 years old. They asked people to show where they lived using a mobile interview of about 15 to 20 minutes in length. Many of the young adults shared feeling highly isolated with very limited in-person interactions—just one to two people on a regular basis in person. And some of the reasons that they shared were because of a lack of accessible places in their neighborhoods that mattered to them, that they wanted to be in, or that they could be in (e.g., were affordable). Other young adults shared that they did not want to engage in drinking culture, so while bars and clubs were aimed at their age group they were not conducive to their lifestyle. They had a lot more strictly online interactions and were less engaged physically in the neighborhood environment. Midlife and later life participants, in contrast, reported being more connected and active in their neighborhoods starting with the pandemic onset, leading to the rediscovery of local places and bonding over shared experiences.
Finlay et al. (2021a) performed mixed methods research to identify specific neighborhood features that may support cognitive health through behavioral social pathways such as physical activity, cognitive stimulation, and social connection. In a qualitative exercise, they asked where and how older adults socialize, exercise, and engage in cognitive stimulating activities outside their homes. This led to developing tailored, customized, and prioritized geospatial measures and hypotheses to test in the REasons for Geographic and Racial Differences in Stroke study. Some examples of places that people said supported physical activity in later life included walkable destinations (e.g., to get groceries or socialize with friends), parks (sometimes small in physical size), and recreation centers (Finlay et al., 2022). Having a greater density of service and amenity businesses, a higher number of parks, and a greater density of recreation centers were all linked positively to cognitive function. Additional analysis found links to performing arts centers and museums, civic and social organizations, and hazards such as highways and polluting sites.
This kind of research can advance understanding of specific neighborhood features and lets researchers inform community interventions, Finlay said.
ADDITIONAL DISCUSSION: DEFINING NEIGHBORHOODS
There was also a discussion about how to implement such definitions of neighborhoods.
- Esposito said that quantitative researchers tend to use what is familiar, and that time constraints and the need to publish get in the way of implementing such approaches.
- Finlay added that there are ways of defining neighborhoods that are less resource-intensive. One way is to carry tablets or even paper maps and ask people to draw boundaries.
- Muñoz commented that almost everyone has a cell phone, and there is a potential for using the GPS data to define neighborhoods, while being careful to respect data sensitivity and identifiability issues.
- Finlay added that another approach is to reverse the narrative by looking at who can be found at particular locations, such as by tracking the zip codes when people use credit cards.
- Esposito commented on the difficulty of generalizing, noting it may be necessary to build interdisciplinary teams for very specific questions. However, it is possible that the work might be simplified based on theory, such as in the discussion of critical periods.
Adina Zeki Al Hazzouri asked for additional discussion of online environments as types of neighborhoods. Finlay responded that this is a new and evolving area. Online environments might be considered as “third places,” with the home being the first place; work and school being the second place; and third places being sites where people gather, connect, and care for each other. It is challenging to measure online environments. Some online data can be analyzed in a quantitative manner, looking for connectivity around something or assessing reviews and comments. There is qualitative evidence that online communities can impact people’s lives meaningfully and form potential pathways from neighborhoods to health. In a recent study one young person used an online gaming platform as a community. For others, local community-oriented sites can be a source of information, though such sites can also have negative impacts, such as when rumors are spread that cause people to avoid certain areas.
Matthew Baumgart of the Alzheimer’s Association asked what risk factors may be associated with neighborhoods, and whether they can be disentangled from positive aspects of an environment. Muñoz responded that she felt they should not be disentangled because they are not truly isolated factors. Rather, Muñoz said they should be looked at in conjunction with each other.







