Identifying Midlife Social Exposures That Might Modify Risks of Cognitive Impairment Associated with Early Life Disadvantage: Proceedings of a Workshop (2025)
Chapter: 2 Laying the Foundation
2
Laying the Foundation
To create a foundation for the later presentations, the workshop started with two presentations aimed at describing how early life disadvantages are associated with later life cognitive decline, how midlife exposures might affect cognitive decline, what data sources currently are available, and what data are needed to support research in this area.
EARLY LIFE RESERVES, MIDLIFE PATHWAYS, AND LATER LIFE DEMENTIA RISKS
Pamela Herd, Carol Kakalec Kohn Professor of Social Policy in the Ford School of Public Policy at the University of Michigan, Ann Arbor, started the discussion, focusing on early life pathways and how they influence midlife risk factors and long-term dementia risk. She noted that there is a robust literature on how early life determinants are related to health in later life, but that the literature is much less robust in discussing cognitive health and especially dementia as an outcome. Influencing health in later life is not necessarily the same as influencing dementia risk. Current theories indicate that dementia risk may be reduced by the building up of brain reserve (or neurobiological capital) and cognitive reserve (the ability to manage “insults” or deal with challenges, such as by finding alternative pathways), while midlife social, behavioral, and health risks lead to an increased likelihood of dementia. This suggests that early life is a critical period for building up cognitive reserve, creating the potential that social and environmental factors can alter cognitive development in early life. During midlife, modifying and/or mediating factors may help to change the likelihood of dementia (Figure 2-1).

SOURCE: Presented to the panel by Pamela Herd on August 29, 2024.
A next question is what factors might affect cognitive development. Herd said multiple factors appear important; they are often interrelated but remain distinct and are not interchangeable. Current data to look at early life factors are best for measuring the relationship between education and dementia, particularly at the individual level (Garcia & Moorman, 2021; Greenfield et al., 2022; Walsemann et al., 2022a, 2024). However, education data may be outdated; people currently in later life grew up in a time when relatively few completed schooling beyond high school, and it is not clear how to extrapolate those data to people getting their education now, when educational levels are substantially higher. Less is known about the impact of factors other than education on cognitive development.
Exploring early life exposures a little further, Herd said there is evidence of the importance of socioeconomic status (SES; Marden et al., 2017; Staff et al., 2012) and of early life deprivation (Zhang et al., 2010). Community conditions associated with dementia include environmental toxins (Lee et al., 2022b), rural location in the first year of life (Herd et al., 2021), and segregation (Zhang et al., 2016). There is robust evidence about how social relationships influence child development and health but less about their influence on later life cognition and dementia.
Herd also emphasized the importance of differentiating between cognitive decline and dementia. There is a robust relationship between educational attainment and dementia but not between educational attainment and cognitive decline. There are also important policy differences. Dealing with some memory loss has fundamentally different implications for a person’s well-being compared with dealing with dementia. Furthermore,
dementias other than AD are often driven by things like chronic health conditions and may be more susceptible to social and environmental influences than AD dementias, which are driven in part by genetic risk. Often there is not clear differentiation in current data between different types of dementia, and better data are needed to develop strong models of what factors influence dementia of each type.
While most individuals with dementia have more than one type of pathology (e.g., AD and non-AD pathology), Herd said AD and non-AD dementias are nonetheless pathologically different and are influenced by differing environmental and biological factors. Hector González (Professor of Neurosciences in the School of Medicine at the University of California, San Diego) commented that the testing process itself is heavily influenced by people’s level of education, and it is difficult to have tests that are not educationally biased. Furthermore, while persons with the APOE-4 gene have elevated risks of AD dementia, there is great variation in how the APOE-4 gene is manifested across racial and ethnic groups, meaning that environmental factors, such as discrimination, may influence how genetic risk for dementia plays out across racial groups. Priya Palta suggested that blood-based biomarkers may be useful for differentiating between AD and non-AD dementias.
Herd said there are many factors of interest in predicting and seeking to affect the risk of dementia. Studies of educational influences are now having their focus expanded from educational attainment to factors such as school resources, the quality of schooling, and school segregation. Another important factor is economic deprivation, including how Supplemental Nutrition Assistance Program (SNAP) benefits (formerly known as food stamps) influence health and mortality. Important community and contextual resources include lead exposure in childhood, rural versus urban environment, pollution, and segregation. Socioemotional resources, such as social connections, social relationships, and nurturing, are known to affect cognitive development, but their long-term influence on dementia risk has not been established.
MIDLIFE MEDIATORS AND MODIFIERS OF EARLY LIFE RISK
Paola Gilsanz, Research Scientist II at Kaiser Permanente Northern California Division of Research, discussed how exposures across the entire life course affect performance on neuropsychological tests. She noted that there can be both direct and indirect pathways of influence. Examples of direct pathways include physiological changes to the brain in early childhood that affect the later risk of dementia. Indirect pathways include early life exposures that may lead to a trajectory of exposures across the life course, which in turn affect late life cognition. For example, education is
thought to have both a direct effect (i.e., building cognitive reserve) and an indirect effect, such as how it influences occupational opportunities, with occupational complexity/stimulation being related to late life cognitive function and dementia risk (Kivimäki et al., 2021; Soh et al., 2023a).
Gilsanz explained that different theoretical models treat direct and indirect pathways differently (Figure 2-2). The life course model that is hypothesized to reflect the underlying causal structure will have implications for what data should be examined and how the findings should be interpreted. There are three primary alternative models:
- In the accumulation model, the early life factor of interest affects the likelihood of dementia directly and also affects midlife exposures that, in turn, affect both the likelihood of dementia directly and also later life exposures, which further affect the likelihood of dementia.
- In the early life critical period model, early life is the only period in which the exposure of interest affects the likelihood of dementia; early life also affects midlife exposures, which affect later life exposures, although exposures in neither of the latter two time periods affect the likelihood of dementia.
- In the pathway model, the early life exposure of interest affects the likelihood of dementia only through its impact on midlife expo
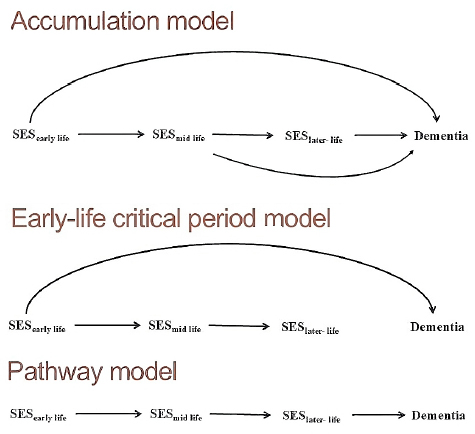
NOTE: SES refers to socioeconomic status, typically measured through a combination of factors such as education, family size, and financial status.
SOURCE: Adapted from presentation to the panel by Paola Gilsanz on August 29, 2024.
- sures, which affect later life exposures, which affect the likelihood of dementia; there are no direct pathways between early or midlife exposures and dementia.
Gilsanz said these models have important implications, as studies often fail to cover all the time periods. Often, if cohort studies start collecting information during midlife, the possible contributions to late life from early-life exposure are missed. Depending on the true underlying causal structure, this can affect the statistical results. Using simulated data, Gilsanz et al. (2022) examined if and, when appropriate, by how much statistical estimates of associations are biased when early life data are missing depending on the causal structure. For example, when the accumulation model reflects the underlying causal structure and the research data start in midlife, Gilsanz et al. (2022) found that midlife and later life estimates were inflated because early life acted as a confounder, while the total lifetime effect was underestimated by 27 percent because the midlife and later life estimates failed to fully capture the effect. When the early life critical period reflected the underlying causal structure, models using exposure data from midlife and beyond produced inflated midlife and late life effects, while the lifetime effect was underestimated by 82 percent. On the other hand, when the pathway model reflected the underlying causal structure, the lack of early life data didn’t affect the direct effect estimates for midlife and later life.
Gilsanz discussed the results of some of the relevant research studies. A pooled meta-analysis of 23 studies showed that individuals with low levels of education had 88 percent greater odds of incident dementia in later life than individuals with high levels of education (Meng & D’Arcy, 2012). Using causal inference methods, one can perform a mediation analysis to examine both the direct and indirect pathways (e.g., through occupation). Comparing high school completion or above with less than high school completion, one meta-analysis estimated a total effect of 1.26 on incident dementia, a direct effect of 1.18, and an indirect effect of 1.06, with an estimated 28 percent of the association between education and incident dementia being mediated by occupational complexity (Hyun et al., 2022). Another study estimated that 11 percent of the risk of incident dementia for those who attended some high school but did not receive a degree was mediated by vascular risk factors, and for those with degrees from graduate schools and professional schools up to 25 percent of the risk was mediated in this way (Liu et al., 2023). Gilsanz noted that the relevance of possible pathways linking exposures to outcomes may vary depending on exposure levels and on their timing.
Gilsanz talked about other factors that need to be considered. The historical context is important, she said, and the meaning or measurement of
key variables such as hypertension and poverty levels may change over time. When looking at the possible impact of education, it is important to consider the history of legalized school segregation in the United States, during which there was systematic under-resourcing of schools designated for Black students. Marginalized students continue to be more likely to attend schools that receive less funding. The timing of an exposure across the life course is also important, and the impact of timing may differ by outcome. For example, one study found that people who attended any college prior to age 30 performed better on tests of executive function than those who attended college after age 30; however, there were no differences between those two groups in performance on tests related to verbal episodic memory (Soh et al., 2023b). The geographic location also matters: people born in a high-stroke-mortality state had higher cumulative incidence of dementia compared to individuals born outside of those states (Gilsanz et al., 2017). Kristen George found that the relationship between birth in the Stroke Belt and late life cognition was attenuated if one accounted for childhood SES and cardiovascular risk factors (George et al., 2021). Community-level SES at both the early life and midlife to late life were associated with later life semantic memory even after accounting for individual level SES (Peterson et al., 2023).
Gilsanz discussed some of the methodological issues in examining a full life course. As discussed earlier, the underlying causal structure matters and influences how important it is to have data over the full life course. Using birth cohorts and early life cohorts (e.g., education cohorts) to examine later life outcomes can require a lot of resources, including the time required for people to age into later life, and possible differential attrition. There may also be concerns regarding generalizability. Another possibility is to embed a cohort within electronic health records or in an integrated healthcare system so that information that was already collected through such records can be linked to the information collected through cohort-specific activities. This option could reduce participant burden by using different sources of data (as opposed to requiring action from the participant), extend the period of time for which there is information on exposures or outcomes, and include repeated measures of exposures or outcomes of interest. As an alternative way of collecting early life data, survey participants can be asked to provide retrospective information, but such data are likely to lack some of the desired specificity and may be impacted by measurement error and recall bias. Differential selection into such studies may also be a concern. In the immediate term, what can be done is to triangulate among the various cohort studies.
DISCUSSION
There was a group discussion of the methodological challenges. Deborah Carr mentioned the potential value for current data collections to also collect data on social media use, treating this as a broad type of social engagement that is social, interpersonal, and cognitive.
A member of the audience asked about international studies in which measures of exposure may have very different meanings depending on the context. Herd and Gilsanz both agreed that it is important to conduct research in international settings and that understanding such contextual factors is very important. Both also felt that there is still much that can be learned by working with what is available in the United States.
There also was a discussion of financial priorities in research: whether it is better to invest in measuring different types of dementia, measure the exposome, or increase the size of the sample. Herd would be reluctant to rely entirely on increasing the sample size but thought the current investment in sample size should probably be increased. Gilsanz suggested that if the sample size is increased, there needs to be attention to how the sample is distributed. Jennifer Ailshire, Professor of Gerontology, Associate Dean of Research and Associate Dean of International Programs and Global Initiatives at the Leonard Davis School of Gerontology at the University of Southern California, commented that the Health and Retirement Study has made this choice, increasing the sample size specifically for underrepresented groups.
This page intentionally left blank.







