Developing an Agenda for Population Aging and Social Research in Low- and Middle-Income Countries (LMICs): Proceedings of a Workshop (2024)
Chapter: 2 The Role of Inequality
2
The Role of Inequality
The first session of the workshop focused on how inequality—in income, wealth, access to opportunities or resources—affects the health and well-being of older populations in low- and middle-income countries (LMICs). Speakers and participants had been given a set of questions to guide their presentations and discussion:
- How does income inequality affect the health and well-being of older populations in LMICs in the context of changing and evolving economies?
- How are changes in the nature of work influencing disability, dementia, and mortality?
- Are there trends, and are they actionable?
INEQUALITIES AMONG OLDER ADULTS IN LATIN AMERICA
In Latin America, older adults experience the burden of infectious and chronic diseases, and the pension, health care, and education systems are not prepared for the changes of an aging society, said Jaqueline Avila (University of Massachusetts Boston). She made the case for studying Brazil and Mexico as a way of understanding the larger region; Mexico and Brazil make up half the population in Latin America, they are the largest economies in the region, and they have large social inequalities. While populations are aging all over the world, the phenomenon is particularly strong in Brazil and Mexico. Compared with the United States, the older populations of Brazil and Mexico are growing faster than the younger populations: see Figure 2-1. This rapid change poses significant challenges, said Avila, especially for the social protection benefits that rely on the contribution of younger individuals. Further, Mexico and Brazil are aging fast in a low-income context; they have much lower gross national income per capita than many other countries. However, by 2050, the share of the population 65 years and older in Brazil and Mexico will be similar, if not greater, than the older adult population in higher-income countries: see Figure 2-2.
There are a number of sources for data to study population aging and health in Mexico and Brazil, said Avila. For Brazil, these sources include the Longitudinal Study of Aging (ELSI), the National Health Survey (PNS), the National Household Sample Survey (PNAD), health data from the national health system (DATASUS), and regional or city-level data. In Mexico, data sources include the Mexican Health and Aging Study (MHAS), the National Survey of Health and Nutrition (ENSANUT), and regional and city-level data.1
Evidence from these datasets shows that older adults in Brazil and Mexico have similar characteristics, said Avila, with comparable rates of chronic disease and similarly low levels of education. In addition, there are common social determinants of health inequalities in both countries, including education, income/wealth, gender, health insurance, and within-country
___________________
1 For more information on surveys, see: ELSI (https://elsi.cpqrr.fiocruz.br/en/home-english/), PNAD (https://www.ibge.gov.br/en/statistics/social/labor/20620-summary-of-indicators-pnad2.html), DATASUS (https://datasus.saude.gov.br/), MHAS (https://www.mhasweb.org/Home/index.aspx), and ENSANUT (https://en.www.inegi.org.mx/programas/ensanut/2018/).
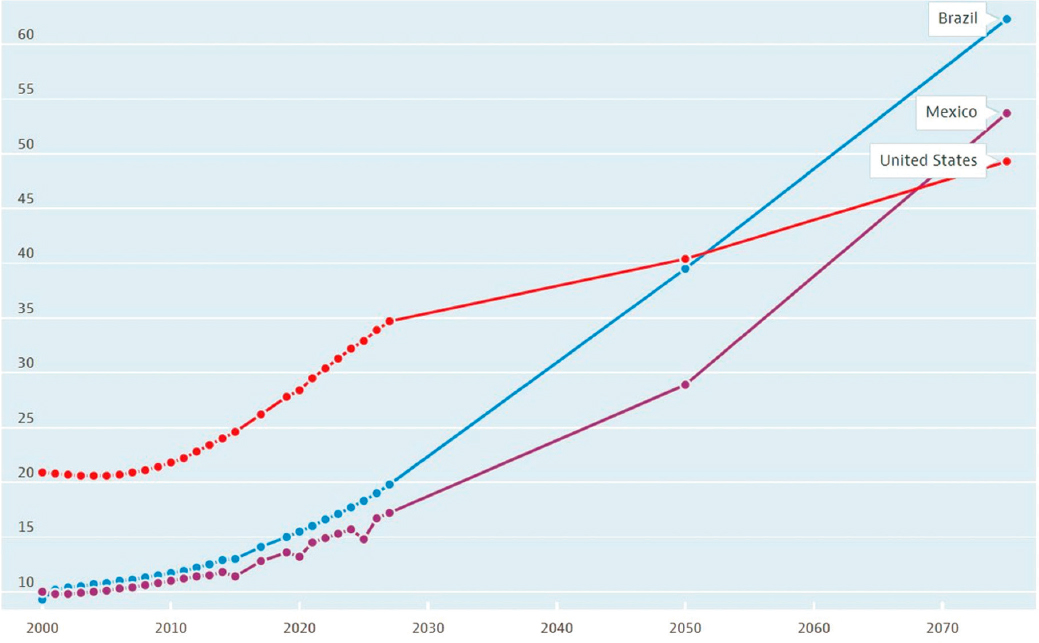
SOURCE: Organisation for Economic Co-operation and Development (2023), Old-age dependency ratio (indicator). https://doi.org/10.1787/e0255c98-en (Accessed on 1 September 2023).
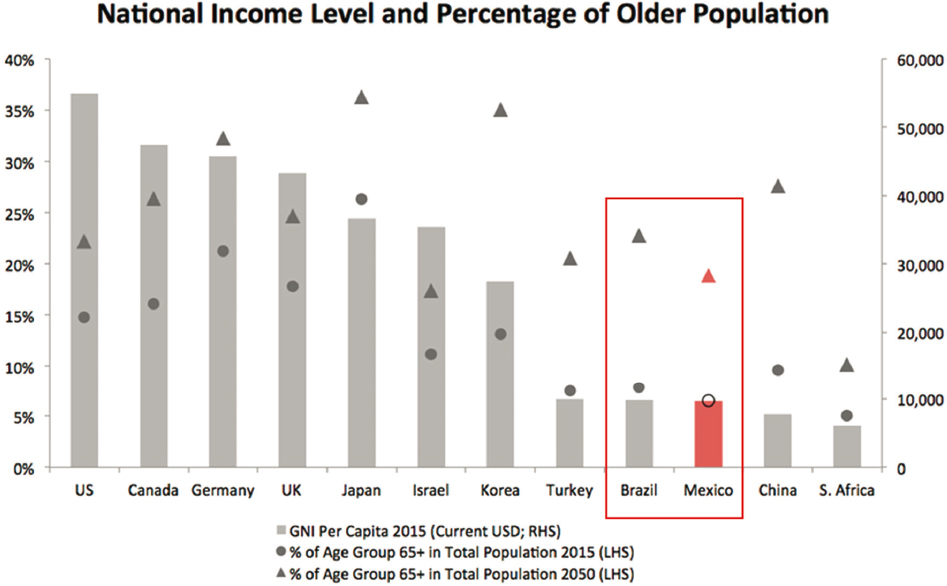
NOTE: RHS, label for right y axis; LHS, label for left y axis.
SOURCE: AARP International (no date, p. 2). Reprinted with permission.
regional differences. Avila detailed how these social determinants affect health inequalities across common risk factors (e.g., tobacco, obesity) and chronic diseases (e.g., diabetes, Alzheimer’s disease and related dementias) in Brazil and Mexico.
Education is the most studied disparity in Mexico and Brazil; both countries have a high proportion of older adults with zero years of education, and functional illiteracy is prevalent even among people with a few years of education. There are also complex interactions between education and gender on health risk factors, said Avila. For example, for men 50 years and older in both countries, the prevalence of obesity increases as education increases. For women, the prevalence of obesity increases along with education in Mexico but decreases as education increases in Brazil. There are large gender disparities in smoking in both countries, with men much more likely to smoke than women. However, the gender gap is closing at every education level in Brazil; and, in Mexico, women with more education are more likely to smoke compared to Brazil.
One clear impact of education for both men and women is in the area of cognitive impairment. Individuals with at least 1 year of education have far lower levels of cognitive impairment than individuals with 0 years of education: see Figure 2-3. However, the benefit of higher education for men in Brazil is lower than the benefit for men in Mexico. The complexity of these data, said Avila, demonstrates the importance of looking at the intersection of multiple characteristics when studying social determinants of health in Latin America.
Income and wealth are also social determinants of large health inequalities in both Brazil and Mexico. Social protection programs, including social security, play an important role in reducing social inequalities for older adults, said Avila. In Brazil, social security is comprehensive and universal; it covers more than 80% of older adults and is the main source of income for them. As a result, there are low levels of poverty among older adults in Brazil. However, she noted that there are challenges ahead due to the increasing old-age dependency ratio: an increasing number of beneficiaries will be relying on a decreasing number of workers. In Mexico, social security is fragmented and tied to one’s employer. People in the large informal work sector do not have access to social security and must rely on supplemental income programs. There are high levels of poverty among older adults in Mexico. Avila said that the different approaches between these countries may give insight on how to best address income and wealth inequalities.
Health insurance systems are another factor that can help narrow health disparities, said Avila. There are major challenges ahead for both Mexico and Brazil, with individuals living longer with a higher prevalence of chronic disease. As with social protection programs, the differences in approaches between Mexico and Brazil may provide insights about the impact
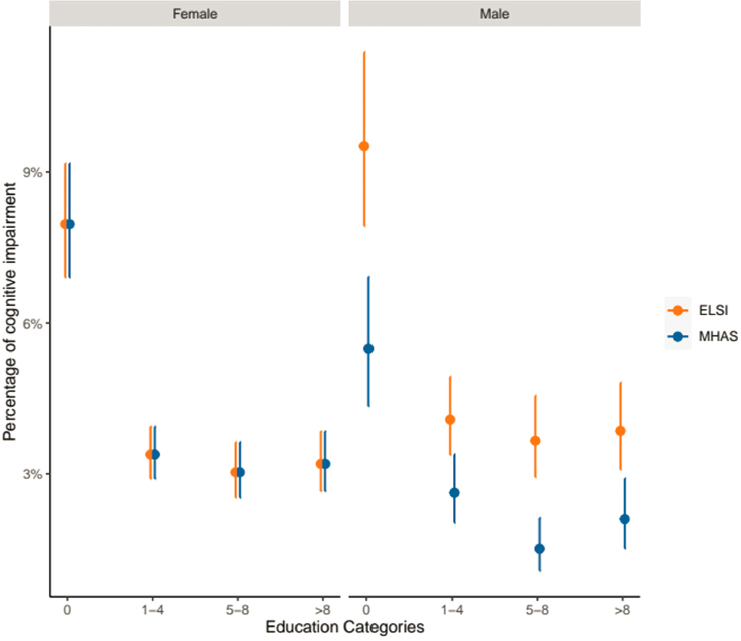
NOTE: ELSI = Longitudinal Study of Aging; MHAS = Mexican Health and Aging Study.
SOURCE: Adapted from Gonçalves et al. (2023, Figures 1 and 2). Reprinted with permission.
of different policy choices. Brazil has universal health insurance, although there are regional differences in good access to care. People with private insurance are wealthier and are more likely to visit specialists than those who rely on public insurance and receive basic primary care. In Mexico, health insurance is fragmented and tied to one’s employer. Before health care reform in 2003, there was a large uninsured population. There have been significant improvements in primary care use and diagnostics, but limited improvements in chronic disease treatment. In both countries, said Avila, the question remains whether the health insurance system is prepared to deal with an aging population with chronic diseases.
When discussing inequality within countries, it is critical to acknowledge that there are important geographical differences and disparities. In Brazil, regional differences are a major source of inequality. Macro-regions are experiencing the pace of the demographic and epidemiologic transition
to an aging population differently, and the North and Northeast areas have poorer access to health care and greater mortality than the South, Midwest, and Southeast regions. In Mexico, differences between urban and rural areas are a major source of inequality. People in rural areas have poorer access to health care, lower education, more poverty, and poorer health than people in urban areas, while people in urban areas have higher rates of obesity and tobacco and alcohol use than those in rural areas.
Across all social determinants, Avila emphasized the importance of studying trends and identifying cohort differences. Studying younger cohorts helps to understand the aging scenario in the coming decades. Social determinants of health inequalities across cohorts are changing fast, and demographic and epidemiologic changes in new cohorts will affect chronic disease burden. For example, obesity prevalence is increasing for men and women in Mexico, and middle-aged adults have higher obesity prevalence than older adults. In Brazil, men with higher education have been quitting smoking, but educated women lag behind in this trend.
Avila closed by identifying several areas to prioritize for research on aging in Latin America, focusing on actionable items with data that are already available:
- leveraging cohort comparisons with cross-sectional and longitudinal data;
- considering multiple social determinants and their interactions;
- using the evidence to promote interventions to decrease regional differences;
- developing methods to validate self-reported conditions; and
- promoting the use of linked longitudinal data with administrative records.
SOCIOECONOMIC STATUS GRADIENTS IN INDIA
Gradients in health are dynamic and change over time, said Nikkil Sudharsanan (Technical University of Munich). However, much of the literature on gradients in LMICs is based on snapshots in time. This gap is due to a lack of available data, but it gives the impression that gradients are static. To illustrate the dynamic nature of gradients in health, Sudharsanan presented data on obesity and associated outcomes in India at different points of time.
A decades-old idea, called the “reverse hypothesis,” posits that cardiovascular risk factors such as obesity are concentrated in the advantaged segments of the population in lower-income countries. As a country develops, the concentration flattens out and eventually flips so that risk factors are more prevalent in the less advantaged segments of society. The limitation
of most research that has tested this hypothesis, said Sudharsanan, is that the research compares countries or regions that are at different levels of development, rather than looking at a single country at different points of time. This kind of comparison relies on a potentially faulty assumption that countries at different levels of development represent what a single country would experience as it develops.
Obesity, Diabetes, Hypertension, and Smoking
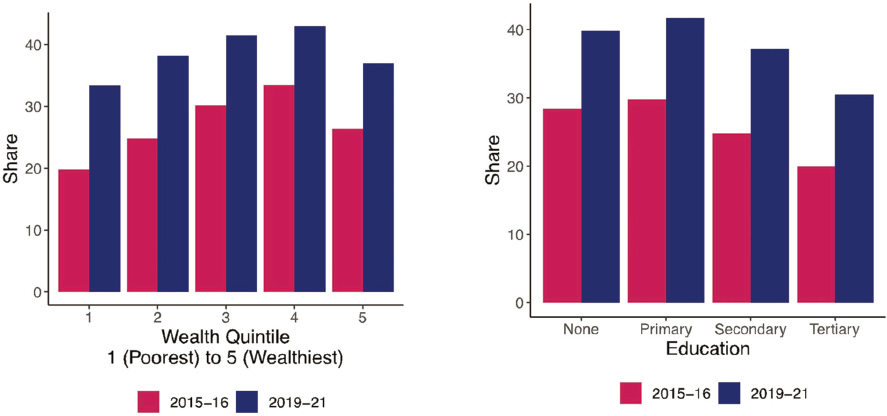
To address this limitation, Sudharsanan and his colleagues looked at gradients in risk factors in India by analyzing data from 2015, 2019, and 2021. They used the National Family and Health Surveys and looked at four outcomes: obesity, diabetes, hypertension, and smoking. The dataset contains over 1.5 million observations, with about 800,000 people per wave.
Sudharsanan said the data on obesity demonstrate a “striking pattern.” Being overweight is much more common among wealthier populations, higher-education groups, and people who live in urban areas. However, the gradients are “flattening in a very short amount of time,” he said. Over a 6-year period, obesity has grown much more in the disadvantaged populations than in the advantaged populations. For example, obesity grew about 8% in urban areas but 30% in rural areas.
The pattern with diabetes is similar, said Sudharsanan. Over the course of the study, prevalence was still higher among the richer populations, but it is shifting over time: the poorest households experienced a 24% increase in diabetes while the richest households experienced a 7% decrease. Sudharsanan noted that patterns can sometimes look different depending on what measure of socioeconomic status (SES) is used (e.g., education, wealth, income).
The reverse hypothesis is most clearly demonstrated with rates of hypertension. The richer populations have higher hypertension, but over the 6-year period covered by the study, richer populations have seen a decrease while poorer populations have experienced an increase. The gradient is “rapidly flipping.”
Smoking is the one risk factor that is more prevalent among the disadvantaged segments of the population, though it is decreasing across all segments. However, similar to the other gradients, smoking has decreased at a much faster rate among more advantaged segments of the population than among less advantaged segments of the population. In this area, the gradient has already flipped and is getting worse over time.
This research, said Sudharsanan, has presented strong evidence in favor of the reverse hypothesis. Over just a 6-year period, rapid changes have occurred in the prevalence of multiple health risk factors, and the trends
are clear. These findings suggest three new questions for future research, he said: (1) Are there contexts where gradients have stabilized, or are gradients always in flux? (2) Given the likelihood that gradients are changing rapidly, how should one look at studies that use cross-sectional snapshots in time to look at inequalities? (3) How do gradients of cardiovascular risk factors interact with health care to produce mortality gradients? Sudharsanan explained that while rates of risk factors are higher among the more advantaged segments of the population, their mortality is not higher; this suggests that access to health care and treatment is moderating the impact of risk factors.
The Effect of Shocks
Based on the idea that gradients can change over time, Sudharsanan and his colleagues set out to understand how shocks can expand gradients. Using National Family Health Survey data from India, they looked at under-5 mortality and over-5 mortality to generate life expectancy estimates by social group and caste. These data were collected both before and after the COVID-19 pandemic began. This inadvertent timing, he explained, allowed researchers to look at pre- and post-COVID mortality, and compare changes among groups.
Sudharsanan and his colleagues found that all groups lost life expectancy after COVID-19, but the loss was far greater among the disadvantaged populations. Between 2019 and 2020, the scheduled castes, scheduled tribes, and Muslims lost around 4 years, while higher caste groups lost only 1 to 1.5 years: see Figure 2-4. An already “pretty striking” mortality disadvantage grew even larger because of the shock of the COVID-19 pandemic, he said. This phenomenon is not unique to India; it was also seen in the United States in expanded mortality gradients by race and ethnicity. It is also not unique to pandemics, he said; disasters such as climate-induced heat or weather patterns often disproportionately affect those who are already disadvantaged.
These findings suggest several intriguing questions for future research, said Sudharsanan. First, are these expansions of gradients inevitable, or are there ways to buffer against expansions? Second, will gradients return to their previous levels, or does the expansion linger or worsen over time?
Policy Challenges to Addressing Inequalities
It is clear there are large inequalities in India, said Sudharsanan. India has worked to address these inequalities through policy and is a “frontrunner” in the area of large social health insurance programs. Around 2007,
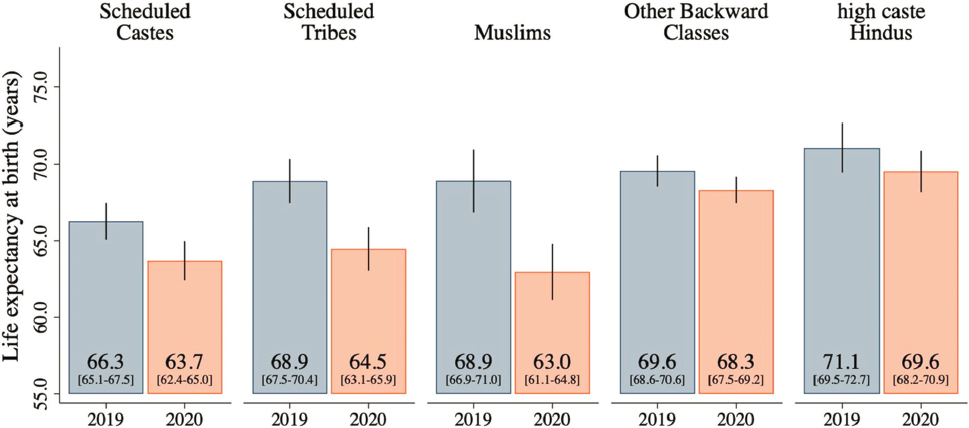
SOURCE: Gupta et al. (2023, Figure 4a). Reprinted with permission.
India implemented Rashtriya Swasthya Bima Yojana (RSBY), which evolved into Pradhan Mantri Jan Arogya Yojana (PM-JAY). Both are government-funded health insurance programs with explicit pro-poor eligibility criteria. The programs seek to overenroll poorer households with the aim of addressing health inequalities. However, these programs have faced major challenges in both targeting and uptake, he said. First, it can be difficult to reliably identify poor households for enrollment. Second, the most disadvantaged groups tend to underenroll, despite their higher need. Working with the Tamil Nadu state government to figure out why tribal populations and urban slum residents are significantly underenrolled in the government insurance program, his colleagues found that it is likely due to “hassle costs”: that is, it is difficult for these groups to find the enrollment sites, travel to the site, and figure out how to enroll.
A recent paper on noncontributory social health insurance coverage in India found that the group that the policy explicitly targets—the poorest quintile—has lower enrollment than other groups (Mohanty et al., 2023). With the transition from the RSBY to the PM-JAY, enrollment increased among all groups: see Figure 2-5. However, the gradient remained, particularly across wealth. When considering policy solutions to inequality, it can be challenging to find a solution that minimizes gradients.
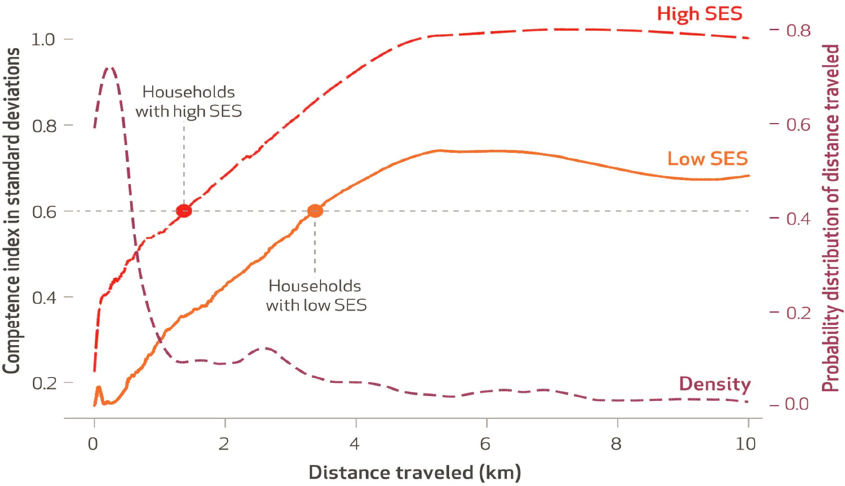
Even if universal health coverage was in place and people from all segments of the population had insurance, there are still gradients when it comes to accessing high-quality health care, said Sudharsanan. A study by Das and Mohpal (2016), looking at how far households had to travel to reach care and how competent these accessible providers were, found that high-SES households can reach a medium-skill provider at a much shorter distance than a low-SES household: see Figure 2-6. Even more striking, he said, is that if high-SES households travel farther, they can reach the most competent providers, whereas low-SES households cannot access these providers even when traveling longer distances. There are challenges in targeting and enrolling low-SES households, and even those who are enrolled face disparities in access to high-quality care.
In conclusion, Sudharsanan offered his thoughts on what is needed to address inequalities. First, he said, we need “non-hand-wavy explanations” for levels and changes in gradients. He explained that researchers spend a great deal of time figuring out how to precisely measure gradients, but then “hand wave our way through why those gradients exist, why they are changing over time, and what we can do about them.” Second, there is a need to closely examine the impact of policies on gradients. There are many policies that have been implemented in India—including public food distribution, caste-based education policies, village health initiatives, and health insurance expansions—that need to be evaluated in terms of their effects on equity. In addition to these policies targeted at the poor, there is a need
SOURCE: Adapted from data in Mohanty et al. (2023, Table 1).
NOTE: SES, socioeconomic status.
SOURCE: Das and Mohpal (2016, Exhibit 4). Reprinted with permission.
to evaluate broad population policies that might affect inequality. For example, taxes on sugar or tobacco, or changes to the built environment (e.g., transportation infrastructure, green spaces) could have an effect on existing gradients; there is a need to research these policies to determine their effects.
RESEARCH APPROACHES FOR INEQUALITY
Will Dow (University of California, Berkeley) discussed research approaches for inequality. There are a few key questions to consider for the research agenda in LMICs, said Dow. First, there has been a great deal of research in high-income countries to understand the mechanisms of how inequality affects health. However, what is unknown is whether these mechanisms operate differently in LMICs. Second is the question of how inequality will evolve in different populations. Finally, said Dow, we need to understand what policy approaches will be most effective in addressing inequality. Dow focused his remarks primarily on income inequality and health, but he noted that there are other important factors that impact inequality and health, including the physical and psychological effects of the changing nature of work.
Dow first addressed the mechanisms that link inequality to health by looking at research largely conducted in higher-income countries. Early research documented that countries with higher inequality have worse population health. There are a number of mechanisms that may be at play, said Dow. First, absolute income improves health, but at a diminishing rate. He explained that if two countries have similar average income, but one has higher income inequality, the more unequal country will have more poverty and worse health. Addressing absolute income is important for reducing the effect of inequality on health, he said.
Another mechanism for the link between inequality and health that has been demonstrated in higher-income countries is a psychological one. Segments of the population with lower incomes experience negative psychosocial effects because individuals compare themselves to others with higher income. A third mechanism, said Dow, is social cohesion. In very unequal societies, the more disadvantaged segments have less social capital, and there is less political support for redistributional policies and society-wide health investments. A key question, he said, is how these mechanisms may or may not operate in LMICs with changing economies.
“Inequality has been with us for a long time, and it is going to be with us for a long time,” Dow said. He shared a graph that shows the share of global income that goes to the top 10%, middle 40%, and bottom 50% of the population over the past 200 years: see Figure 2-7. However, while inequality has historically been between countries, it is now primarily within countries: see Figure 2-8. This pattern means that it is critical to collect
data within countries that include details on individuals across the income spectrum, rather than relying on national averages. Another major change that has occurred is a sharp increase in the female share of labor income because of increased education and rising participation in formal labor markets. Dow said that this is an important area to continue to study; specific foci could include whether the work of women in nonmarket settings is or is not changing and how these trends affect inequality and health.
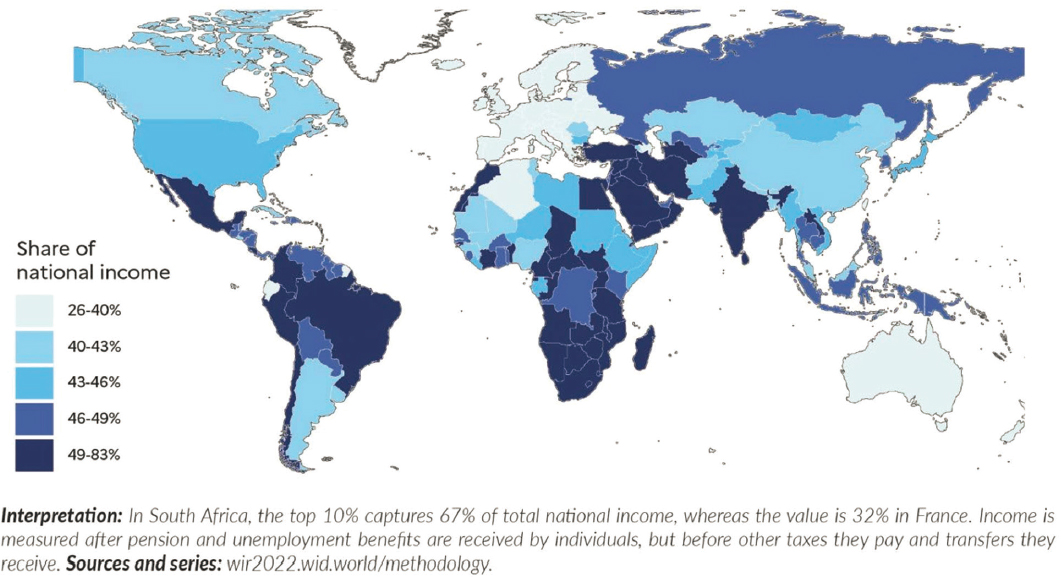
Income inequality is higher in LMICs, said Dow, with the top 10% of the population earning over half of the national income in many countries, including South Africa, India, and Brazil: see Figure 2-9. With higher inequality in these countries, there is a larger need for policies to address inequality and its associated risks, he said.
Dow discussed three main types of policies aimed at mitigating SES gradients in health: first, taxing the high-income/wealthy segments of the population to fund poverty reduction, which is a “politically difficult proposition in many countries”; second, investing in programs that shift health upward for the entire population; and third, buffering the negative health consequences of low SES by providing interventions to this population. These types of social spending rose dramatically in Europe over the 20th century, with spending on health care, pensions, education, justice, social transfers, and other programs rising from around 10% of gross domestic product (GDP) in 1915 to 45% of GDP in 1980.
While it is difficult to know how each type of expenditure has affected health, the rise of the European welfare state “arguably has had a huge impact on health outcomes in European countries,” he said. In contrast, tax revenues and social spending in LMICs are far lower. In sub-Saharan Africa and South and Southeast Asia, tax revenue is under 20% of GDP, and spending on health care and education are less than 3% each. However, there are some LMICs that have been spending much more significantly on social programs. For example, Costa Rica has a very robust social safety net, and it has a smaller SES gradient in health than the United States. Even more striking, said Dow, is the fact that the bottom socioeconomic quartile of the Costa Rican population has better health than the bottom quartile of the U.S. population.
While large public investments are clearly needed in order to make an impact on inequality and health, said Dow, the ability to make these investments is constrained by an ongoing shift from public to private wealth. Over the last 50 years, private wealth has been increasing dramatically in high-income countries, while public wealth—the sum of financial and nonfinancial assets, net of debts, held by governments—has decreased at the same time: see Figure 2-10. Dow said the same trends are occurring in most LMICs, though not yet as dramatically.
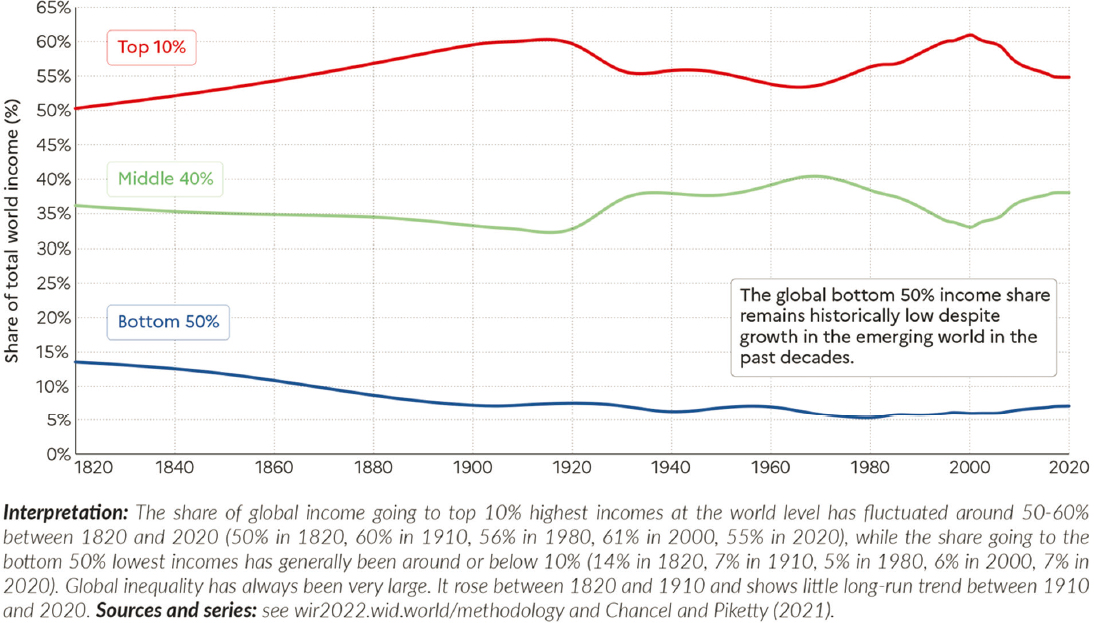
SOURCE: Chancel et al. (2022, Figure 2.1). Reprinted under Creative Commons 4.0 (https://creativecommons.org/licenses/by/4.0/) on behalf of World Inequality Lab, https://inequalitylab.world/en/
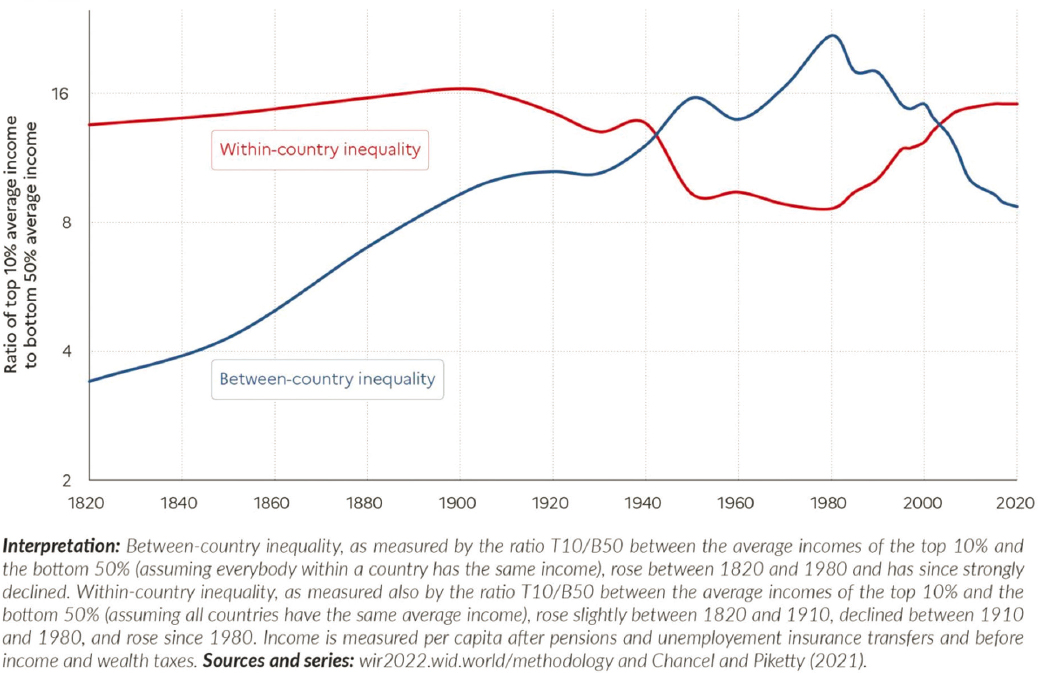
SOURCE: Chancel et al. (2022, Figure 2.4). Reprinted under Creative Commons 4.0 (https://creativecommons.org/licenses/by/4.0/) on behalf of World Inequality Lab, https://inequalitylab.world/en/
SOURCE: Chancel et al. (2022, Figure 1.6a). Reprinted under Creative Commons 4.0 (https://creativecommons.org/licenses/by/4.0/) on behalf of World Inequality Lab, https://inequalitylab.world/en/
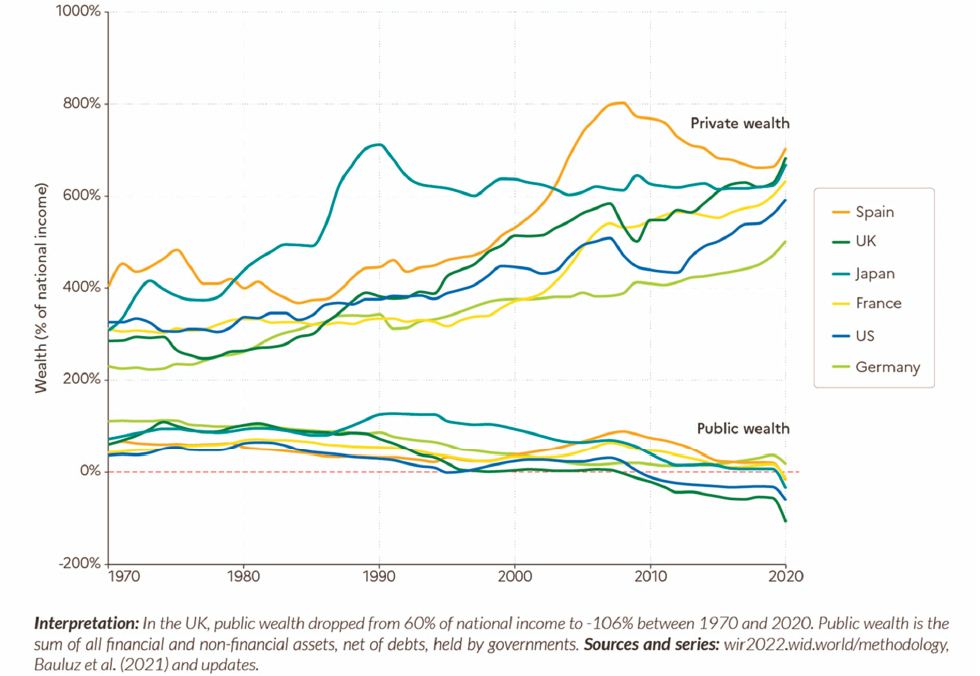
SOURCE: Chancel et al. (2022, Figure 3.2). Reprinted under Creative Commons 4.0 (https://creativecommons.org/licenses/by/4.0/) on behalf of World Inequality Lab, https://inequalitylab.world/en/
In conclusion, Dow suggested three approaches to research that should be prioritized. First, there is a need to build on cross-national research by using harmonized surveys across LMICs and high-income countries in order to test hypotheses on inequality, health, and policy. This type of research is necessary, he said, because there are not usually “beautiful natural experiments” in which it is easy to see causation between a policy and a health outcome. Second, there is a need for research on specific policy changes or interventions in different LMIC contexts in order to grow the generalizable knowledge base. This will require more investment in LMIC surveys, as well as building research capacity in LMICs. Finally, there is a need for macro-level approaches that capture general equilibrium feedbacks. For example, the National Transfer Accounts project has begun incorporating inequality as an element in order to look at the impacts of demographic dividends and their relationships on changing health in more than 60 countries. This will require more investment in macro-level research and macro-level researchers, said Dow.
DISCUSSION
Following the speakers, Minki Chatterji (National Institute on Aging) moderated a question-and-answer session with speakers and participants. She began by summarizing the sessions’ presentations. Inequality remains a problem, and there are implications for health. We have some idea of the causal mechanisms through which inequality leads to adverse health outcomes, including tobacco use, obesity, diabetes, and access to care, Chatterji said. However, these mechanisms are still “a little bit fuzzy,” particularly in LMIC contexts. There is a need for research on mechanisms in LMICs, as well as on different policies and how they lead to different outcomes. Chatterji asked panelists to comment on two questions related to these needs. First, why is this research not happening with the data that already exist? Second, are the data and infrastructure in place to do this research, and if not, what is needed?
Avila responded that the answers to these questions vary by country. For example, there are a lot of data for Mexico, but more are needed in other countries. For countries that have significant data, a lot could be learned by linking longitudinal datasets with administrative-level data. One reason that this has not yet been done, she said, is that the data are relatively recent so “we are still kind of catching up.”
Sudharsanan offered his perspective from working in India. Administrative data are often not available, are of poor quality, or are difficult to obtain. Even something as basic as data on health care claims do not exist, he said. The lack of data means that researchers have to “let go” of the goal of a comprehensive, “satisfying” micro-causal estimate. He added that
the incentives in public health are often geared toward quicker, easier types of research that can “generate ten publications” from one dataset. There is a need, he said, to find ways to reward deeper types of inquiry that take more time.
Dow agreed that it can be very difficult to get access to data, in part because many countries do not have a culture of data sharing. This is beginning to change, but more efforts are needed to encourage and support data sharing. In other countries, in particular in sub-Saharan Africa, the data are simply not available. There is a need to invest in the data that will be necessary to evaluate policy changes. In addition, Dow said that more work is needed on building capacity. He said that the mechanisms for supporting scholars and researchers in LMICs are underdeveloped and frequently not well matched to the needs of the scholars.
Yaohui Zhao (Peking University; workshop planning committee member) agreed with the need for capacity building and said that there is a need to work with countries on what kinds of incentives are provided to researchers. For example, most grants have certain restrictions on how money can be spent, and these restrictions may be in conflict with the constraints and incentives for researchers from certain LMICs. There is a need to align incentives in order to facilitate easier collaboration among researchers across country lines.
This page intentionally left blank.





















