Developing Multimodal Therapies for Brain Disorders: Proceedings of a Workshop (2017)
Chapter: 2 Multimodal Therapy: Overview of Principles, Barriers, and Opportunities
2
Multimodal Therapy: Overview of Principles, Barriers, and Opportunities
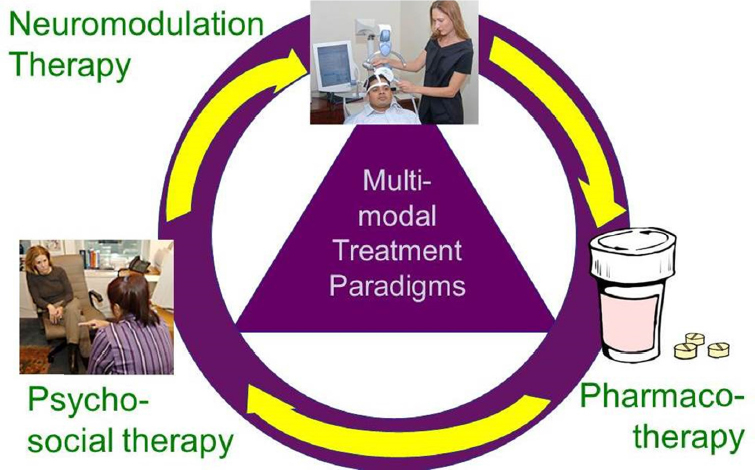
Multimodal therapies are intended to optimize treatment of brain disorders by delivering different types of therapy together. The multiple modes used may include pharmacotherapy (small molecule drugs and biologics), devices, and behavioral/psychosocial interventions (see Figure 2-1). These different modalities may target a particular neural system (e.g., a drug plus neurostimulation), or one modality may be used to activate or potentiate a neurological circuit so that the other modality can have a therapeutic effect.
An overarching theme that emerged from the workshop was that to effectively develop multimodal therapies, a sophisticated understanding of disease processes and disease phenomena is needed, said Karl Kieburtz. A second major theme, raised by FDA commissioner Califf, relates to the challenge of achieving the scale needed for trials in the neurosciences by reducing costs and improving efficiency. Multimodal therapies increase the complexity of this challenge because evidence is required about both the independent and combined contributions of constituent modes across practice, regulatory, and reimbursement decision-making contexts, said Kieburtz.
DEFINING MULTIMODAL THERAPY
This workshop generally considered “multimodal therapy” as a broad category that involves combining two or more modalities that target different aspects of a disease. During workshop discussions, however, it was clear that there is no single set of terminology used across the
field and that there is partial overlap among various commonly used terms.
“Combination therapy” is frequently used to refer to two or more drugs or biologics used in combination—either to enhance delivery of a drug or target different aspects of a disease, or to improve outcomes toward the same aspect of a disease—and also sometimes used to refer to approaches involving multiple modalities.
A “combination product,” according to the FDA definition, is one that combines two or more types of medical products that may be differently regulated. These may be two different components combined into a single entity, such as a drug-eluting stent, co-packaged as a kit or sold separately and labeled for use together (see Box 2-1). Some—but not all—combination products involve combining modalities to target different aspects of a disease. Conversely, some multimodal therapies do not meet the formal definition of a combination product, for example, because one component is not a regulated product, such as psychotherapy.
For clarity in this document, “multimodal therapy” is used except when discussing drug−drug combinations or when specifically referencing a product that meets the FDA’s formal definition of a combination product. Importantly, although they did not meet the working definition of a multimodal therapy, the workshop included discussion of drug−drug combinations and FDA-defined combination products that do not address different aspects of a disease, because such approaches have been developed further and involve similar challenges; therefore, lessons learned may be applied to multimodal therapy development.
SOURCE: Presentation by Lisanby, June 14, 2016.
RATIONALE FOR MULTIMODAL THERAPIES IN BRAIN DISORDERS
Several workshop participants noted that the lack of efficacious therapies for numerous neurological and psychiatric disorders, as well as diminishing returns from the addition of new monotherapies, have fueled the pursuit of multimodal therapies. Moreover, in other disease areas, such as cancer or HIV/AIDS, the use of combination therapies has dramatically improved the treatment of disease.
Multimodal approaches may combine therapies that alone have only modest effects, but have dramatic effects when put together. For example, in coronary artery disease, the multiple modes used may include a drug-eluting stent; multiple pharmacologic therapies, including blood thinners, statins, antihypertensives, and biologics; and behavioral interventions, such as diet and exercise. Multimodal approaches (as well as some combinations of multiple drugs) also offer the potential to target different pathological mechanisms simultaneously according to a number of presenters at the workshop. For example, in PD and Alzheimer’s disease (AD), protein misfolding and dysfunction in how proteins are trafficked and cleared, neuroinflammation, mitochondrial dysfunction, oxidative stress, and other aging pathways have all been implicated and may need to be targeted in combination. Some workshop participants pointed out that there may be additive or synergistic effects of combined therapies. Even a drug that has an insignificant effect when used as monotherapy may be effective when combined with another agent. For example, carbidopa by itself has no impact on PD symptoms, but is used in combination with levodopa to prevent peripheral metabolism of levodopa so more of it can reach the brain
Multimodal approaches are also often necessary for conditions such as traumatic brain injury (TBI), which has multiple consequences, including cognitive disability, psychological injury, behavioral disorders, sensory disturbances, and pain; it is also accompanied by other visceral and orthopedic injuries (see Figure 2-2). Similarly, there is much more to PD than motor symptoms, including the possibility of cognitive impairment, autonomic dysfunction, sleep dysregulation, and pain.
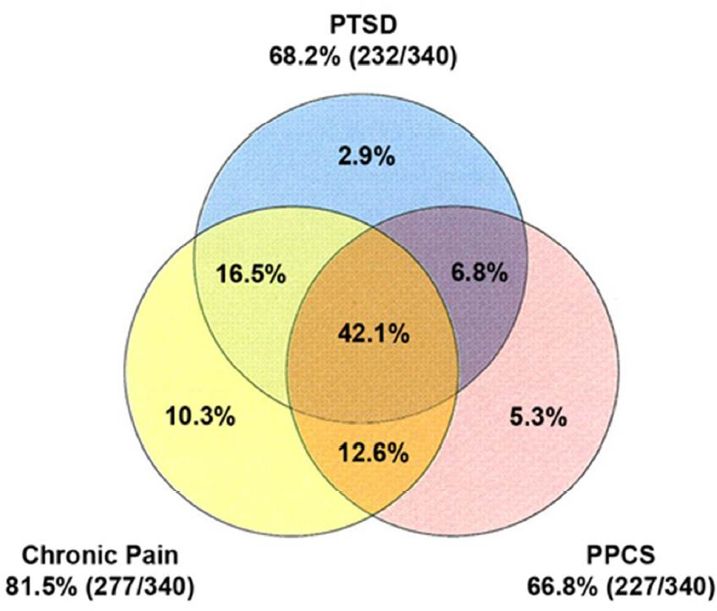
SOURCE: Presentation by Hoffman, June 15, 2016.
Multimodal approaches may enable more individualized, targeted treatment. For example, for a highly heterogeneous condition such as epilepsy, pharmacotherapy may be combined with continuous monitoring of brain electrical activity and neurostimulation to prevent seizures. Indeed, multimodal therapy is commonly used in clinical practice and often recommended in professional practice guidelines, even though there are many cases in which the combinations have not been methodically assessed. For example, medication plus cognitive behavioral therapy is the standard of care for depression.
CHALLENGES AND BARRIERS
The challenges of getting a single drug approved are magnified in the development of multimodal therapies, said James Hendrix, director of global science initiatives at the Alzheimer’s Association. These include an insufficient understanding of the underlying neurobiology of the diseases, inefficient trial designs, and unclear regulatory and marketing pathways. While non-pharmacologic therapies may be important components of multimodal therapies, these are in some cases even less well understood than are the pharmacologic components.
Stevin Zorn, president, CEO, and co-founder of MindImmune Therapeutics, Inc., noted that current cost constraints demand the development of more efficient drug development pathways. Timothy Strauman, professor of psychology and neuroscience at Duke University, added that novel and complex research designs, treatment protocols, and statistical algorithms are required to translate insights from neuroscience and cognitive science about the pathophysiology of complex disorders and potential treatment mechanisms of action into improved treatments, including multimodal and personalized medicine approaches. This chapter provides an overview of barriers and opportunities identified by individual participants; these topics are discussed in greater detail in later chapters.
Insufficient Understanding of Disease and Treatment Mechanisms
To effectively and efficiently develop multimodal therapies, a sophisticated understanding of disease process and disease phenomena is needed, including linking target engagement to a biological response, tracking the trajectory of a disease over time, understanding risk phenotypes, and understanding the mechanism of action of the intervention, noted Kieburtz, Zorn, and Keith Hildebrand, senior principal scientist and technical fellow for neuromodulation at Medtronic, Inc. Yet as noted by Amir Tamiz, program director of the NIH Blueprint Neurotherapeutics Network, limited preclinical models for central nervous system diseases make it difficult to develop a specific monotherapy, let alone combine therapies and understand whether there is an additive or synergistic effect.
For complex and heterogeneous diseases with multiple mechanistic pathways, such as PD, there is also a need to understand the interactions
of these multiple pathways, said Kieburtz and Brian Fiske, senior vice president for research programs at The Michael J. Fox Foundation for Parkinson’s Research (MJFF). An incomplete knowledge of mechanisms also translates into lack of knowledge about what markers could and should be measured, including early biomarkers that predict a later response to treatment, noted Lisanby and Hildebrand.
Non-pharmacologic therapies are an important component of many multimodal approaches, yet the details of how such therapies work are poorly understood, said Lisanby. For example, for neuromodulation, insufficient knowledge about how the delivered dosage (composed of the spatial distribution of the induced field and the temporal dynamics of the field) and the context in which the field is administered (composed of brain state at time of stimulation, phase of neural oscillations, and concomitant cognitive-behavioral interventions and pharmacotherapy) interact at a mechanistic level represents a research gap that impairs the ability to optimize the efficacy of multimodal therapies, she said.
Translating Acquired Knowledge to Scale for Effective Multimodal Therapies
The challenge of translating new discoveries into effective treatments useful in real-world settings is also exacerbated for multimodal therapies due to insufficient scale, according to Califf. He added that stakeholders have not identified mechanisms to create the scale needed to bring down costs and truly understand how various treatments interact or could cumulatively interact for more effective treatments. Lisanby added that neuroscience trials frequently have a small sample size and are statistically underpowered to detect a signal for each component part, which impedes scale-up and examination of the components combined. Kieburtz added that for chronic diseases, a lack of proximate measures to what are often long-term outcomes result in lengthy trials and limit the use of adaptive designs and other trial design innovations that may be needed for multimodal therapies.
Complexity of Trial Design Needed to Assess Multimodal Therapies
Hendrix highlighted some of the challenges faced when testing multiple therapies in combination. These include demonstrating the pharmacodynamic and pharmacokinetic properties of multiple compounds,
determining the correct doses of the compounds in light of possible additive or synergistic effects, and assessing potential drug−drug interactions. The route of administration (e.g., oral versus infusion therapy) adds further complexity to dosing strategies and regimens, he said.
Dose is particularly challenging in trials of non-drug approaches. For neuromodulatory therapies, quantifying dose requires consideration of parameters across three dimensions: spatial distribution of the induced field, temporal dynamics of the field, and the context in which the field is administered, which is affected by what the person is thinking or doing, who is in the room, environmental conditions, stress, etc., said Lisanby and Martha Morrell, chief medical officer at NeuroPace and clinical professor of neurology and neurosurgery at Stanford University. Morrell added that the effects of neurostimulation may require months or even years to fully manifest, making it difficult to design a trial of reasonable duration that will truly represent treatment efficacy.
For psychosocial interventions, quantifying dose has typically relied on measures such as number of contacts with a therapist and duration of treatment; however, other factors that are less easy to quantify also affect dose, such as applied treatment techniques (e.g., exposure, cognitive restructuring, and emotion regulation) or the therapeutic alliance, interpersonal functioning, and variability among practitioners, said Wolfgang Lutz, professor and head of clinical psychology and psychotherapy at the University of Trier, Germany, and Marom Bikson, professor of biomedical engineering at The City College of the City University of New York.
Obtaining Regulatory Approval for a Multimodal Therapy
Establishing the safety and effectiveness of a single therapy in order to gain regulatory approval is challenging, and adding other components to a trial increases the complexity and difficulty of achieving approval, said Hendrix. Kieburtz and Lisanby added that the challenge is exacerbated by separate regulatory pathways and different evidentiary standards for drugs, biologics, and devices. Moreover, no regulatory framework exists for behavioral interventions or other psychosocial therapies, said Kieburtz and Strauman, including components such as neurocognitive tasks, brain-training games, and cognitive-behavioral therapy, added Lisanby.
Billy Dunn, director of the FDA’s Division of Neurology Products at the Center for Drug Evaluation and Research (CDER), said that with drug−drug combinations, each component must make a contribution to
the overall effect, and there should be a compelling reason to use the drugs in combination. Wilson Bryan, director of the division of clinical evaluation and pharmacology/toxicology at the Center for Biologics Evaluation and Research (CBER), added that if multimodal therapy combines a drug or biologic plus an unregulated intervention, such as a psychosocial intervention, the same standards of evidence apply as would apply to the drug alone.
Payers’ and Regulators’ Perspectives on Multimodal Therapies
The high cost of medical care is forcing difficult decisions to the forefront for payers, providers, and patients, and multimodal therapies may be escalating those costs, said Rhonda Robinson-Beale, senior vice president and chief medical officer of Blue Cross Idaho. She said that payers often require comparative effectiveness studies, which Kieburtz noted are not part of the FDA framework for approval. Moreover, said Lisanby, regulators and payers often have different evidentiary standards for efficacy and safety across modalities.
As the scientific understanding of multimodal therapy evolves, reimbursement issues need to be addressed in early stages of development, said Lisanby. A particular challenge for developers, noted Califf, is that conducting one set of studies for regulatory approval and a whole different set of studies for payers is an inefficient use of resources. Another concern for developers is that if a multimodal therapy is shown to be more effective than monotherapy, this could lead to payers incentivizing or requiring the use of the intervention in the multimodal rather than monomodal context, noted Lisanby.
Complexities and Challenges in Bringing Multimodal Therapies to Market
In addition to the technical and scientific challenges of developing multimodal therapies, companies face commercial challenges in bringing those therapies to market, particularly because multimodal approaches often involve multiple companies as well as multiple modalities, said Califf. For example, companies or investors may be reluctant to pursue development of multimodal therapies because of concern about treatment interactions. If multiple treatments are to be evaluated in a single trial, a company may refrain because they fear their treatment will lose out to an
alternative. There is also little commercial incentive for companies to participate in head-to-head trials.
Hendrix added that few companies are large enough or have sufficient resources to conduct combination or multimodal trials in-house and thus must rely on collaborations with other companies, which present further complications. Intellectual property concerns represent a barrier to multimodal therapy development, said Tamiz.
POTENTIAL OPPORTUNITIES TO ADVANCE MULTIMODAL THERAPY DEVELOPMENT1
According to Strauman, the fields of cognitive psychology and cognitive neuroscience are on the verge of a paradigm shift, with the increasing ability to target specific dysfunctions in particular neurologic circuits. To effectively tackle the many complexities and realize this potential, said Lisanby, innovation is needed at all levels: in trial design, analytic approaches, and partnerships across stakeholder groups. Following is an overview of the opportunities raised by individual workshop participants. These opportunities are explored further in later chapters.
Advancing Understanding of Disease Mechanisms and Treatments
Throughout the workshop, individual participants identified a number of areas where additional research on the fundamental aspects of neurological diseases could advance the development of multimodal therapies. These include
- Research that envisions and generates multimodal therapies that hit different targets, similar to the way heart disease is currently treated (Koroshetz).
- Clinical research aimed at promoting multimodal therapy that targets at-risk populations for early intervention and prevention (Edwards).
___________________
1 These lists highlight topics discussed throughout this workshop, but should not be construed as reflecting a consensus of workshop participants or any endorsement by the National Academies of Sciences, Engineering, and Medicine or the Forum on Neuroscience and Nervous System Disorders.
- Research to develop short-term markers that are objective and quantifiable and that could predict long-term change in a variety of conditions, including pain and complex behavioral disorders such as depression (Lisanby).
- Research to develop targeted interventions for behavioral manifestations of conditions that traditionally have been considered neurological, such as mood dysregulation, sleep disturbances, anxiety, and agitation in TBI, AD, and PD (Lisanby).
- Research to optimize parameters for neuromodulatory devices across three dimensions: spatial distribution and temporal dynamics of the induced field and the context in which the field is administered (Lisanby).
- Research targeting behavioral manifestations such as agitation in the context of AD, and nonmotor symptoms such as cognition in PD (Fiske, Hendrix). This includes developing a better understanding of whether symptoms share a common underlying biologic substrate or if there are multiple mechanisms, and whether these symptoms are epiphenomena or core features of the disease.
Improving Efficiency Through Trial Design Innovations
- For co-development of pharmaceutical agents, using innovative trial designs—including adaptive trials, 2 × 2 factorial designs, and fractional factorial designs—could offer efficient ways to accurately detect and quantify the synergistic or additive effects of treatments (Kieburtz, Lewis).
- Incorporating statistical modeling and response adaptive randomization could enable resources to be shifted toward approaches that appear most promising (Lewis).
- Building platform trials could enable the efficient exploration of the effects of multiple treatments in heterogeneous populations over extended periods of time (Lewis). For example, a transdiagnostic approach for drug discovery could exploit the overlap between all neurodegenerative diseases (Hendrix), or neuropsychiatric diseases through the Research Domain Criteria (RDoC) initiative of NIMH (Lisanby).
Identifying Measures and Biomarkers for Improving Clinical Trials
- Identifying and validating measures of target engagement in precompetitive space could enable drugs to be tested against biologically rational mechanisms before initiating large, expensive Phase III trials (Koroshetz).
- Identifying and validating biomarkers that demonstrate a clinically relevant response to treatment could potentially provide a single readout for combination trials in AD (Hendrix).
- Developing tools for estimating drug exposure in the brain to enable interpretation and understanding of outcomes in clinical trials (Potter).
Improving Data Gathering, Data Sharing, and Data Analysis
In addition to improving the design of clinical trials, innovative analyses and methods for obtaining and disseminating relevant high-quality data are particularly important for multimodal therapy because of the increased complexity of these approaches, according to some workshop participants. Ideas discussed at the workshop include the following:
- Capturing data from electronic health records and integrated health systems could provide opportunities to achieve the scale and real-world data needed for successful clinical trials (Califf, Edwards, Pizer).
- The FDA, with the cooperation of industry, is moving toward using existing data from clinical trials and common data standards to increase the scale of studies of multimodal therapies for central nervous system (CNS) disorders, as is already being done in oncology (Califf, Potter).
- Using innovative approaches to data analysis through crowd-sourcing and contests could expedite development and expand the community of researchers exploring multimodal therapy (Hicks). Prize models may also encourage the participation of investigators from diverse disciplines, including quantitative analysts from the financial world (Kieburtz).
- Incorporating big-data methods and large-scale analytics could allow investigators to capture and learn from devices already
-
used in clinical practice, such as long-term ambulatory electrocorticographic (ECoG) monitoring (Morrell).
- Calling for people to enable their data to be used by researchers to answer questions and volunteer for trials, a major focus of the Precision Medicine Initiative, offers the potential for gathering large quantities of data from heterogeneous populations (Califf).
- Improving training of the next generation of neuroscientists, including data scientists, and reeducating students and scientists about the range of options for study design and data analysis are essential for continued progress in the field (Strauman).
De-Risking Multimodal Therapy Development Through Collaborations
- Building a collaborative consortium of competing companies to tackle preclinical and infrastructure issues in precompetitive space could help move multimodal drug development forward (Hendrix).
- Addressing intellectual property issues by ensuring that each partner receives benefits from innovative partnerships could help mitigate the risk of such partnerships (Zorn).
- Providing research funding at the federal level and from private funders focused on particular diseases can play an important role in de-risking drug development, for example, by investing in head-to-head trials for which there is no commercial incentive for companies (Lisanby), or promoting the repurposing of drugs for combination therapy (Hendrix).
- Developing programs for head-to-head trials to develop evidence across modalities, which incorporate provider/professional organizations and patients (Califf, Lisanby).
This page intentionally left blank.













