Biological Threats and Terrorism: Assessing the Science and Response Capabilities: Workshop Summary (2002)
Chapter: Appendix H NACCHO Research Brief: Assessment of Local Bioterrorism and Emergency Preparedness
Appendix H
NACCHO Research Brief: Assessment of Local Bioterrorism and Emergency Preparedness
INTRODUCTION
“Is the United States ready for a bioterrorist attack?” This is a question continually posed by concerned citizens and the media. Local public health agencies (LPHAs) serve on the frontlines in responding to bioterrorism threats and other public health emergencies. LPHAs play a key role in preparing jurisdictions for bioterrorism, including rapid detection of unusual health events, coordination with response partners and healthcare facilities, providing treatment recommendations and protocols to prevent spread of infection and disease, doing “contact tracing” to assure that all individuals exposed to bioterrorism agents are reached for testing and treatment, and providing health information and resources to the public and the media.
The threat from bioterrorism has become more real since the recent September 11, 2001, terrorist attacks on the United States and recent anthrax incidents. These incidents have led many LPHAs to examine their capacity to prepare for, detect, and respond to emerging health threats. The National Association of County and City Health Officials (NACCHO) conducted a survey in October 2001 to assess local preparedness for bioterrorism and found that only 20% of LPHAs have a comprehensive response plan in place. LPHAs have made progress and learned important lessons about the challenges of bioterrorism preparedness in the last few years, but have a long way to go to achieve the capacities needed to detect and respond to an act of bioterrorism as quickly as possible, to prevent the spread of disease and save lives.
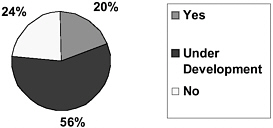
FIGURE 1: Percent of LPHAs with a Comprehensive Response Plan.
METHODOLOGY
The data presented in this research brief were obtained from an assessment of LPHA bioterrorism and emergency preparedness conducted by NACCHO. In response to the September 11, 2001, attacks and subsequent anthrax incidents, NACCHO conducted this survey to better understand how these events impacted LPHAs and how prepared they were to respond. A 9-question survey was developed by NACCHO, and was faxed and e-mailed to 999 NACCHO members and state associations of local public health agencies. In a short turnaround time of one week, 530 responses were received, a response rate of 53%.
Once survey responses were received, NACCHO staff conducted the data analysis. Open-ended questions were coded for ease of analysis, and data analysis was conducted using the statistical software package Stata®.
LPHAS IN THE AFTERMATH OF SEPTEMBER 11
Local health officials played a variety of roles in response to the September 11 terrorist events. Most of these roles revolved around communicating with various partners within their communities. A number of respondents indicated that much of the time was spent fielding questions from concerned community members and staff. Other roles included working with response partners to develop, update, and review plans and protocols to respond to emergencies. Developing fact sheets and providing information to the public and media were also mentioned.
Other roles mentioned by respondents included placing LPHA staff on alert, activating or supporting emergency operations centers (EOC) community systems, activating emergency response plans, and increasing disease surveillance. Some respondents indicated that they had to rely on the news media to be alerted and receive updates, not local disaster response agencies, state health departments, or federal agencies.
When asked how well prepared the LPHA was to play these roles, 15% indicated they were well prepared, while a large majority, 75%, said they were only fairly or somewhat prepared. Nine percent (9%) of respondents indicated they were not prepared at all.
TYPES OF INQUIRIES RECEIVED AS A RESULT OF THE ATTACKS
Sixty-six (66%) of LPHAs surveyed indicated that the health department received a significant number of questions regarding the September 11 event or terrorism/bioterrorism in general.
By far, most inquiries received were questions concerning vaccination and medication availability. Other frequently asked questions dealt with the level of local preparedness and the existence of emergency response plans. Many citizens wanted to know how prepared their community was, what the LPHA was doing to prepare the community, and how they could obtain copies of the local plan. There were also numerous questions regarding the threat of bioterrorism, such as: “What is the likelihood that a bioterrorist attack would occur?” and “Are we in danger of crop sprayers spreading bio-agents?” Lastly, there were questions about where the community would receive necessary resources and where citizens could donate blood or help in any other way.
When asked how well prepared they felt to respond to these inquiries they were receiving, 38% of the LPHAs who responded indicated they were “pretty well prepared” to respond, while another 50% said they were only “somewhat prepared,” and 12% felt they were “not prepared at all.”
FRUSTRATIONS AND LESSONS LEARNED
Many LPHAs indicated they faced several problems and frustrations in this time of crisis. The chief frustration voiced by respondents was the lack of resources and equipment failure. Specifically, many discussed the malfunctioning of necessary communication tools such as pagers, cell phones, e-mails, and faxes. This frustration was related to the second most frequently reported frustration: lack of or poor communication from state and federal agencies. Many local health officials interpreted this lack of information as poor leadership from federal and state health agencies.
Another common frustration was about insufficient local preparedness. Many LPHAs indicated they lacked a fully developed response plan. Others had no plan at all. Other frustrations included lack of consistent and standard information regarding bioterrorism, poor coordination between public health and emergency management, and the need for increased training among LPHA staff and the need for more specialized staff. Problems dealing with the media, such
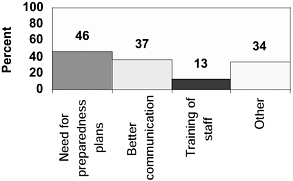
FIGURE 2: Percent of LPHAs: Lessons Learned
as countering incorrect media information and being overwhelmed with questions from the media, were also cited as common frustrations.
Sixty-four percent (64%) of the LPHAs surveyed indicated that the events of September 11 contributed some lessons learned for their health department (see Figure 2). The primary lesson was that they are not adequately prepared for a bioterrorist attack and that they need to have a response plan in place with clearly defined roles and chain of command. There is also a need for enhanced collaboration among federal, state, and local agencies, including development of up-to-date contact lists. Furthermore, many realized the importance of reliable methods of communication, including pagers, cell phones, email. The need to train LPHA staff was also noted. Other lessons learned dealt with improving syndromic surveillance capacity, addressing mental health issues, and providing information to physicians, the public, and the media.
CONCLUSIONS
Gaps in local public health preparedness were clearly realized in the aftermath of September 11. Our nation’s local public health system is lacking in its preparedness to protect its communities if faced with a biological attack. Bioterrorism preparedness plans, effective communication systems, and reliable and timely information are key to a prepared public health workforce, yet these pieces are currently incomplete.
Additional resources to enhance our nation’s public health system are critical at this time. LPHAs play a vital role in the response to bioterrorism and other emergency situations. The capacities needed by LPHAs to effectively respond to an act of bioterrorism allow for the development of a dual-use infrastructure that improves the capacity to respond to all local public health emergencies and hazards. NACCHO will continue its efforts to build local response capacity to benefit and improve the health of communities nationwide.
NACCHO is the national organization representing local public health agencies (including city, county, metro, district, and tribal agencies). NACCHO works to support efforts which protect and improve the health of all people and all communities by promoting national policy, developing resources and programs, and supporting effective local public health practice and systems.
This report was prepared by Anjum Hajat, MPH, Zarnaaz Rauf, MPH, and Carol Brown, MS.




