Understanding and Preventing Violence, Volume 2: Biobehavioral Influences (1994)
Chapter: Some Areas Not Addressed - Some Roads Not Traveled
that began with a group of pregnant women. Significant correlations between maternal alcohol ingestion during pregnancy and the attention performance of the child at age 4 have been reported (Streissguth et al., 1984). This finding was replicated and extended to other cognitive behaviors at age 7 1/2 (Streissguth et al., 1986, 1989). This study provides strong presumptive evidence that the roots of academic failure (and later delinquency) may lie in maternal drinking (even of moderate amounts) during pregnancy.
Cocaine, Opiates, and Tobacco Data now exist (Table 17) showing that maternal use of cocaine has a significant depressant effect on reflexes and state control in infants and a general impairing effect on neonatal neurobehavioral capacities (Chasnoff and Griffith, 1989; Chasnoff et al., 1985). Although the children in such cohorts may be too young to allow reliable assessment of cognitive capacities, it seems reasonable to assume that many of them may present significant academic and social problems as they develop and enter the school system. In more or less the same vein, Table 17 summarizes some recent reports of reviews of later effects in the child of maternal use during pregnancy of opiates (Olofsson et al., 1983; Wilson et al., 1979) and tobacco (Rush and Callahan, 1989). It should also be noted that Streissguth found nicotine effects on performance in her maternal alcohol studies independent of alcohol effects (Table 16).
Some Areas Not Addressed—Some Roads Not Traveled
In the course of this review of neurobiologic factors of possible relevance to the development of aggression and violence, it became evident early that the literature on related factors or related clinical populations was staggeringly large and could not be addressed in a single paper of this size. The areas chosen for discussion are obviously in part a reflection of the interests and biases of the authors; other authors would probably have chosen to emphasize different aspects of the problem and would have made different selections from the voluminous related literature. The following list of undoubtedly relevant problems, factors, or clinical groups either has not been discussed in this review or has been mentioned so fleetingly as to have been essentially ignored:
Attention deficit disorders, with or without hyperactivity
Social learning of violence
Autonomic nervous system influences
Neurochemical factors
Neural specificity/plasticity
Kindling of seizure foci
The issue of whether or not human aggression and violence can be linked unequivocally to disordered brain mechanisms remains very much in doubt. The literature surveyed in this report is suggestive of some relationship between pathophysiologic processes in the limbic system and the tendency to engage in assaultive and violent behavior; however, the issues of sample size, sampling bias, and the co-occurrence of other variables that could account for the excess violence in the patient or offender groups under study remain for the most part unresolved. Although it is true that many studies of violent persons have found evidence of brain abnormalities, the possible role of a violent lifestyle (leading to head injuries) is generally difficult or impossible to control. Violent lifestyles, moreover, for many young male residents of impoverished areas, may be adaptive or at least difficult to avoid. The role of parental mistreatment leading to injury, not only to the brain but to self-esteem, also needs to be considered: violence begets violence. Possibly, there is one issue that can or should be laid to rest: violence occurring in the course of a seizure (ictal violence) is an almost nonexistent phenomenon.
In the course of this review, a number of suggestions were made that could simplify the process of doing research in this area and help to clarify the relationship of brain disorders to aggression, violence, and other types of antisocial behaviors. One would involve the creation of a national health registry of the type that exists in a number of Scandinavian countries. This resource has, in fact, been exploited in a most profitable manner by many American and Scandinavian researchers to illuminate and clarify the role of nature and nurture in the development of schizophrenia spectrum disorders (Rosenthal and Kety, 1968). Data from the police or court systems would automatically be entered into the registry. This would allow us to ascertain, with some assurance, the actual prevalence and incidence of antisocial, as well as other, behaviors in various populations at risk. The necessary precautions would have to be observed to restrict access to the data to qualified researchers, and to prohibit the use of the information for any purpose other than research. This is virtually identical to the recommendation made by one of the authors in 1974 (Mirsky and Harman, 1974:204):
Only large scale survey data with competent, standardized reporting of neurologic, psychiatric and behavioral information will permit us to describe adequately the relation between epilepsy, temporal lobe disease and disordered social behavior. … And the potential additional information would insure the value of the project. For example, if an association were found between aggressive, violent or other socially unacceptable behavior and a series of neurologic, demographic and environmental variables, then a prospective study could be done in which a group of infants or young children at risk for such complications in later life could be extended every medical, environmental and social benefit. A matched control group without such advantages would be constituted that would not receive such comprehensive ministrations, and the outcome of the two groups could be evaluated at 5, 10 and 15 years. If the treatment were successful in preventing or reducing the development of unacceptable behavior, it could then be extended … to all children at risk.
It may be possible to implement a less grandiose and utopian scheme by performing population-based surveys in one or more cities. Such surveys have been conducted by the National Institute of Mental Health (NIMH) for the purpose of identifying persons with psychiatric disorders and have been useful for mental health planning. Subjects at risk could be identified in this way, and controlled studies involving various types of interventions could be launched. Interventions could include training targeted at improving general classroom competence, as implemented by Kellam and Rebok (1992) in the Hopkins-Baltimore preventive intervention project (see below) or aimed at specific cognitive weaknesses such as attention and concentration. While it is true that violent acts may be relatively rare, their occurrence may reflect a much more prevalent and widespread problem associated with disordered cognition: failed academic opportunities, underachievement of occupational level, increased nonviolent (as well as violent) crimes with the attendant staggering costs of courts and jails.
We believe that this review has highlighted the fact that violent behavior is more likely the consequence of impaired cognitive processes than of altered emotional states. Our efforts should therefore be directed toward understanding, controlling, ameliorating, and reducing the effects of brain-damaging environments.
Some modest efforts along roughly these lines have been undertaken by NIMH in the creation of prevention intervention research centers. One of the authors (AFM) is collaborating with the staff at the Department of Mental Hygiene at Johns Hopkins University and is involved in the planning, assessment, and evaluation
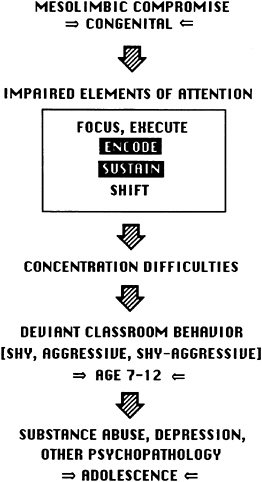
FIGURE 6 This model is based on data gathered in the course of the collaborative Johns Hopkins University—NIMH prevention intervention research project referred to in the text, as well as the results of the studies by Kellam and colleagues (1975) in the Woodlawn district of Chicago.
of cognitive-based interventions. A tentative model, based on some of the preliminary results from this collaboration, is included in Figure 6. The model starts with the assumption of early congenital damage to limbic or related mesencephalic structures of the brain. This in turn leads to difficulty with certain "elements of attention" (Mirsky, 1989) in elementary school, and thence to teacher-identified concentration difficulties and early academic failures. These may result in deviant classroom behaviors (shyness, aggressiveness, shyness and aggressiveness in combination)



