Assessing the Burden of and Potential Strategies to Address Antimicrobial Resistance: Proceedings of a Workshop—in Brief (2024)
Chapter: Assessing the Burden of and Potential Strategies to Address Antimicrobial Resistance: Proceedings of a Workshop—in Brief

Assessing the Burden of and Potential Strategies to Address Antimicrobial Resistance
Proceedings of a Workshop—in Brief
There is broad recognition that the spread of antimicrobial resistance (AMR) is a significant and evolving threat to public health. A global, systematic analysis estimated that in 2019, 4.95 million deaths were associated with AMR (Antimicrobial Resistance Collaborators, 2022). However, there is uncertainty as to whether the impact of AMR is fully understood and measured across the spectrum of medical practice and in other relevant sectors, such as food production. To address this question, the Forum on Microbial Threats of the National Academies of Sciences, Engineering, and Medicine held a 2-day virtual workshop on March 4–5, 2024, to assess challenges and share strategies to address the growing worldwide threat of AMR. Speakers presented on assessing the burden of AMR; investigating the impact across different medical specialties; monitoring AMR in plants, animals, and the environment; and discussing the extent to which the impact of AMR is being quantified. Sessions also focused on improving strategies to address AMR through stewardship, drug access, and other innovations.
SURVIVING ANTIMICROBIAL RESISTANCE
Anthony Darcovich, member of the World Health Organization (WHO) Task Force of AMR Survivors, shared his journey as a survivor of AMR. An injury from playing baseball first led to a rotator cuff surgery, followed by a number of additional operations when the shoulder pain was not relieved. Finally, he was diagnosed with an infection of clindamycin-resistant Cutibacterium acnes, a common skin commensal bacteria. Over the next 9 months, he underwent eight surgeries; multiple debridements that damaged the joint and cartilage leading to the need for shoulder reconstruction; and daily intravenous infusions to clear the infection. Darcovich highlighted that even a common bacterium like Cutibacterium acnes has led to decades-long ramifications for his health, significantly compromised his quality of life, and likely will continue to factor into his future health care. He notes that there can be a tension between patients who seek antibiotics to resolve infections quickly and clinicians who may be conservative with prescribing antibiotics, but he hopes that patient voices and considerations are included in discussions on how to address AMR. For example, morbidity is critical to quality of life for survivors of AMR but is often underemphasized by the medical community, he pointed out. He hopes that the Task Force of Survivors will allow patient perspectives to be heard when considering solutions for addressing this evolving threat.
STRATEGIES TO ADDRESS ANTIMICROBIAL RESISTANCE ACROSS MEDICAL PRACTICE
Susan Huang, medical director of epidemiology and infection prevention at the University of California, Irvine,
![]()
discussed the high risks of infection faced by nursing home residents. Millions of nursing home infections occur annually, and a 2019 study estimated that 64 percent of nursing home residents carry at least one multidrug-resistant organism (MDRO), such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), or extended-spectrum beta-lactamase producers (McKinnell et al., 2019). The high MDRO prevalence is driven by shared activities and spaces, higher chronic illness prevalence, and poor quality cleaning and bathing. These drivers can be countered with better cleaning practices, contact precautions, improved hand hygiene, and decolonization, said Huang. In particular, decolonization can greatly reduce the risk of MDRO infection, she explained, and is especially beneficial to patients during high-risk periods, such as after surgery or when skin is fragile from rashes or wounds. Decolonization of the skin with chlorhexidine gluconate (CHG) is more effective than simply cleaning with soap and water, as it is able to kill bacteria over an extended period of time, and the benefits of decolonization practices have been documented in hospitals, after discharge, and in nursing homes.
Huang shared results from her 18-month study in skilled nursing facilities that demonstrated that the use of decolonization methods with nasal iodophor and chlorhexidine antiseptic soap during routine bathing significantly reduced the presence of MDROs compared to using just soap and water (Miller et al., 2023). Nursing homes in the intervention group saw a 17 percent decrease in infections as a cause of hospitalization and a 31 percent decrease in the rate of infection-related hospitalizations, suggesting that decolonization is an effective strategy for reducing AMR in skilled nursing facilities, Huang said. However, she noted that significant challenges exist in developing new decolonization treatments owing to the lack of a clear research and development pipeline and ambiguity around the Food and Drug Administration (FDA) approval process for decolonization agents.
Shawn Rangel, professor of pediatric surgery at Harvard Medical School, shared his experiences with antimicrobial overuse in hospital surgical settings. Rangel cited a meta-analysis estimating that up to 50 percent of pathogens causing surgical site infections may be antimicrobial resistant (Teillant et al., 2015), and he suggested that these numbers will continue to increase. Two programs, the National Surgical Quality Improvement Program (NSQIP) and the Children’s Surgery Verification (CSV) program, were developed to compare adverse events such as surgical site infections (SSI) among hospitals nationwide. A joint benchmarking report by the American College of Surgeons and NSQIP reviewed surgical antimicrobial prophylaxis (SAP) and SSI rates across the country and found that there was no correlation between overuse of SAP and the rate of SSI—demonstrating that increased use of prophylactic antibiotics did not lower SSI rates (He et al., 2022). Rangel further shared that a 2021 NSQIP-Pediatric report revealed overuse of antibiotics at Boston Children’s Hospital, particularly in postoperative prophylaxis patients. Since the overuse of antibiotics did not lead to decreased SSI rates, this report encouraged the hospital to reduce antibiotics use in postoperative patients.
In 2023, an updated report showed the hospital had significantly decreased use of antibiotics and become one of the low users of all the hospitals evaluated (American College of Surgeons, 2022). Rangel pointed to this as an exemplar of how data and accountability from annual, nationwide comparative benchmarking can promote stewardship and practice modification at the institution level. In closing, Rangel said surgical prophylaxis is only one of many areas where comparative benchmarking can facilitate antimicrobial stewardship, and he encouraged the implementation of similar practices in other areas, such as treatment of established surgical and nonsurgical infections and the use of antimicrobial prophylaxis for medical conditions.
John Wingard, oncologist and professor emeritus at the University of Florida Medical School, highlighted the significant effect of AMR on cancer patients. He said infection is one of the most common complications of oncology treatment and the second leading cause of death of cancer patients (Zheng et al., 2021). Contributors to the high risk of infection include the patients’ impaired immune responses and harmful effects of chemotherapy. Wingard noted the association of infection with the onset of febrile neutropenia following chemotherapy and that patients with solid tumors have different risks of infection and AMR than those with hematologic malignancies. Patients with solid tumors account for 90 percent of cancer patients and have lower
![]()
risk of febrile neutropenia compared to hematologic cancer patients (Freifeld et al., 2011). Thus, antibiotic prophylaxis is more often recommended for patients with hematologic malignancies because of their higher risk of neutropenia, bacteremia, and infectious mortality. Evidence suggests that this prophylaxis results in decreased febrile episodes, decreased documented infections, and lower mortality rates (Gafter-Gvili et al., 2012). However, he noted this practice also leads to an increase in AMR in both pediatric and adult cancer patients, particularly in E. coli and VRE infections (Nanayakkara et al., 2021).
Wingard discussed some strategies that can reduce AMR infection rates. For example, antibiotic deescalation can reduce the frequency and duration of broad-spectrum antibiotics use, and baseline predictors of bacteremia can be used to tailor antibiotic use. In addition, infusions of engineered myeloid progenitor cells can be used to reduce infection, and promising research has explored new approaches to using probiotics to lessen the deleterious effect of antibiotics on the gut microbiome. In conclusion, Wingard said oncologists need new rapid diagnostics and AMR detection assays to guide decision making for this vulnerable patient group, as well as multicenter clinical trials to validate these emerging strategies for reducing AMR.
MONITORING AMR IN PLANTS, ANIMALS, AND THE ENVIRONMENT
Joakim Larsson, director of the Center for Antibiotic Resistance Research in Gothenburg, Sweden, explained the environment’s role in AMR development and spread. Larsson stated that the environment acts as vast reservoir of new resistance genes that over time end up in pathogens, and that certain pathogens (e.g., fecal bacteria) are often transmitted to humans and animals via the environment. His recent research suggested that wastewater is an enabling environment for the development of resistance in bacteria. Larsson suggested that the key to controlling AMR may be to determine when resistance genes become mobile and how they spread between organisms (Berglund et al., 2023).
While antibiotic use is a recognized driver of AMR, lack of sanitation and transmission control boosts the spread and is likely to be an even more important driver on a global scale, Larsson said. Since poor sanitation results in high levels of both resistant and nonresistant fecal bacteria (such as E. coli) in receiving waters, simply measuring total E. coli concentrations in treated wastewaters may be a resource-efficient surveillance method to assess transmission risks, he said. Larsson added that benchmarks for comparison are required for surveillance systems to be beneficial. Western countries may provide the best benchmarks for low AMR levels because of their good clinical surveillance systems, he said, and these benchmarks can be used to predict clinical resistance in areas of the world that may lack sophisticated clinical surveillance but bear much of the burden.
Paul Plummer, associate dean of research and graduate studies at Iowa State University College of Veterinary Medicine, discussed challenges in sharing AMR data across One Health sectors, using the example of differences in clinical breakpoints for AMR in humans and animals. Clinical breakpoints are used to determine resistance levels and guide treatment decisions for specific antimicrobials used for a specific species. However, Plummer pointed out that clinical breakpoints for the same bacteria may differ between patient or host species. For example, ampicillin is used to treat E. coli infections in humans and cattle, but it is administered in different doses at different frequencies in human and in cattle, thus the clinical breakpoints for resistance are different in these two use cases and cannot be directly compared. Plummer emphasized the need to create a common measurement system for antimicrobial susceptibility between human and animal health, and he suggested using epidemiologic cutoff values to determine if a specific bacterial isolate has acquired resistance. Epidemiologic cutoff values can provide comparable metrics for both humans and animals because they are independent of host and drug factors (e.g., dosing interval, administration route).
In closing, Plummer cautioned that in many cases, measuring resistance using clinical breakpoints developed for a single patient species cannot be used across One Health sectors. When asked about the role of conducting antimicrobial susceptibility testing (AST) prior to the use of antibiotics to avoid treatment failure, Plummer explained that there are significant economic challenges around AST testing. For example, it is difficult to convince clients to do a $200 AST test when giving antibiotics treatment for the issue costs significantly less, he said. He stated that investment in early diagnostics to reduce
![]()
testing costs is critical to increase the prevalence of AST testing before treatment.
Ken Opengart, vice president of animal welfare and international sustainability at Tyson Foods, shared his experience managing the health of broiler chickens in a commercial food animal production setting. Tyson Foods operates in a vertically integrated system, where the company maintains ownership of the birds at various farms and provides veterinary oversight. Caring for animals on this large scale is challenging, he said, particularly managing bacterial diseases with limited effective treatments. Tyson Foods follows guidance from both WHO and the World Organization for Animal Health (WOAH) to determine which antibiotics to use in response to issues that arise at individual broiler chicken farms.
In 2017, the company eliminated the use of antibiotics in their broilers, designating them “No Antibiotics Ever.” However, this practice ultimately led to negative effects on both the animals and farmers, and in 2023 Tyson Foods transitioned to a “No Antibiotics Important for Human Medicine” approach, which allowed antibiotics approved for use in animals only. This switch increased broiler chicken livability, improved animal welfare, and reduced disease incidence. Opengart concluded that while there may be years when antimicrobial use increases because of higher disease incidence in the broiler flock, Tysons’ decision focused on reducing the overall need for antimicrobials and keeping animals healthy. Finally, Opengart shared that Tyson Foods is also focused on reducing the need to use antibiotics in general through the use of prevention efforts such as vaccination, sanitation, and worker training programs.
SURVEILLANCE AND POTENTIAL PREVENTION MEASURES
Olga Tosas, infectious disease epidemiologist at WHO, presented ongoing efforts to improve AMR data surveillance methods. The Global Antimicrobial Resistance and Use Surveillance System (GLASS) was founded in 2016 and collates AMR data from 135 countries for 13 bacterial pathogens and 32 antibiotics across 11 antimicrobial classes. However, Tosas shared that factors such as differences in access to diagnostics, finances, and levels of diagnostic stewardship limit the extent to which AMR surveillance data can be compared and interpreted across countries. To address these limitations, Tosas shared a new two-pronged approach that has been successfully applied for HIV and tuberculosis surveillance. This approach uses a combination of data collection from routine clinical sampling and complementary strategies such as patient surveys to improve data quality and representativeness, she said. Tosas advocated for the use of periodic surveys in AMR and shared how surveys, especially case report forms on hospital patients with bacterial infections, can be used to collect information on the prevalence, economic burden, and health effects of AMR.
The same data collected in parallel from a control group of uninfected patients also provides insight on health and economic burden metrics such as excess mortality, disability-adjusted life years, and years of life lost in that community. Tosas noted that colonization data can provide useful information about a potential infection, and WHO is working to learn if colonization data has public health value in predicting disease burden and resistance levels, with the eventual goal to predict infection levels on a population level. In closing, Tosas said this two-pronged AMR surveillance model can help generate nationally representative and comprehensive data on antimicrobial, health, and economic burdens, as well as improve quality standards that allow data to be comparable across countries and time.
Dawn Sievert, senior science advisor for antimicrobial resistance coordination and strategy at the U.S. Centers for Disease Control and Prevention (CDC), discussed strategies employed by CDC to address AMR. CDC monitors AMR in the United States through multiple data sources, she said, to provide information on pathogens, human infections, and risk measurements, which are then used to estimate cost, burden, and AMR mortality rates. CDC uses a three-category system to keep track of AMR pathogens that pose a risk to morbidity and mortality, she said. Criteria such as medical impact, economic impact, number of treatment options, and transmissibility are considered when categorizing pathogens as either a concerning, serious, or urgent threat.
CDC’s Antimicrobial Resistance (AR) Threats Report presents data on these priority pathogens, along with information on the effects of investments in the AR space. Domestically, CDC has built lab capacity by fitting regional and state labs with new technology and validated testing
![]()
methods to enhance testing capacity in every state. The AR Lab Network has increased resource capacity and communication with state and public health officials to inform local responses to emerging threats. CDC is also improving lab detection and response to high-level AMR threats globally through its Global AR Laboratory and Response Network. Both the domestic and global networks focus on pathogens identified in the AR Threats Report.
Sievert highlighted recent advances in AMR surveillance and monitoring, such as electronic reporting and ordering systems that allow for automated real-time data sharing, decreased turnaround times, and quicker responses. However, she argued that more extensive AMR data tracking and sharing beyond acute health care settings is needed, in addition to measurements of health equity for identifying risk factors among vulnerable and high-risk patient populations. Finally, she called for increasing focus on stopping transmission in health care settings and better global data sharing to mitigate the increasing spread of AMR.
Joseph Lewnard, associate professor of epidemiology at the University of California, Berkeley, reviewed how the burden of AMR can be reduced through infection prevention efforts. In response to a question about the role of providers overprescribing in AMR, Lewnard shared that changing provider prescribing practices is a complex process involving cultural and technological challenges. Patient expectations for rapid treatment is compounded by diagnostic uncertainty and often results in prescribing antibiotics. He pointed to three types of interventions that are especially effective in preventing infection and reducing AMR-associated deaths across high-income countries (HICs) and low- and middle-income countries (LMICs): (1) vaccination; (2) water, sanitation, and hygiene (WASH) interventions; and (3) infection prevention and control measures in health care settings.
WASH interventions have been successful in preventing some antibiotic-treated conditions, with hand hygiene specifically having the potential to reduce the incidence of nosocomial (health care–acquired) infections—a large source of AMR burden, Lewnard said. He called for increased focus on vaccine usage worldwide and noted that reduction in antibiotic use in HICs has been achieved through the prevention of acute infection rather than decreasing antibiotics prescriptions. He also advised that improved infection prevention and control standards, such as hand hygiene, could prevent thousands of deaths in LMICs.
Suzanne Young, technical officer of global coordination partnerships in the AMR division of WHO, presented on the Quadripartite collaboration for multisectoral action on AMR.1 She shared that the goal of the quadripartite joint secretariat on AMR is to preserve antimicrobial efficacy and ensure the sustainability, equitable access, and responsible use of antimicrobials. Young described the governance structure of the secretariat, which includes the Global Leaders Group (GLG) that was formed in 2020 as a high-level advocacy group for AMR. GLG contributed to ensuring that AMR commitments made at the September 2024 United Nations General Assembly are specific and identify accountable stakeholders to facilitate implementation.
GLG also aims to build on the 2016 UN declaration, which faltered in achieving its targets because of a lack of sufficiently specific goals and follow-up actions, Young said. Currently proposed targets for 2030 from the GLG include reducing global AMR deaths by 10 percent, reducing the use of antimicrobials globally in the agri-food system by 30–50 percent, and eliminating the use of antimicrobials important for human use in animals for nonveterinary purposes and crop production. GLG also recommends that each country develop its own outcome-oriented and sector-specific targets with clear goals and timelines for addressing AMR, Young said.
ANTIMICROBIAL STEWARDSHIP
Kristin Ray, pediatrician at the University of Pittsburgh Medical Center Children’s Hospital, discussed challenges and opportunities for antimicrobial stewardship in outpatient telehealth care. Telehealth encompasses a variety of care models, and requires attention to the specific technology, people, and processes involved in a given model in order to achieve high quality care, she said. The use of live interactive telehealth increased significantly during the COVID-19 pandemic and facilitated health
__________________
1 The Quadripartite is a collaboration of the World Health Organization, the Food and Agriculture Organization, the United Nations Environmental Programme, and the World Organization for Animal Health that works to address One Health issues. See https://www.qjsamr.org/ (accessed August 23, 2024).
![]()
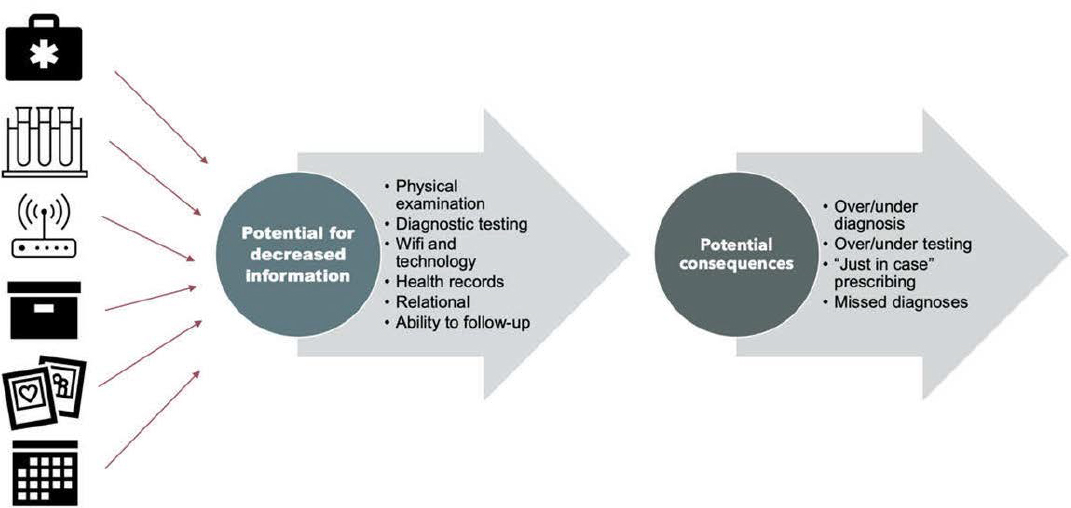
SOURCE: Kristin Ray presentation, March 5, 2024.
care access. The rise in telehealth use brought increased attention to the potential challenges of telehealth, including limitations on information available in some virtual visits compared to traditional in-person evaluations, Ray explained (Figure 1).
She also highlighted opportunities to enhance information in virtual visits through specific tools, technology, and processes. During the early pandemic period when stay-at-home orders were in place, antibiotic prescribing during telehealth visits was higher compared to the later pandemic period, when telehealth could be used in a more hybrid model of care (i.e., clinicians could use telehealth or in-person options to care for their patients). With this increase in telehealth use, there is a need to attend to antimicrobial stewardship in outpatient telehealth care, which requires attention to appropriate metrics, information exchange, and communication strategies, Ray stated.
Building on this conversation, Ray highlighted opportunities to improve antimicrobial stewardship during telehealth visits. She highlighted recent work translating the CDC’s four core elements of antimicrobial stewardship into virtual care spaces: establishing standards for telehealth diagnostics and antibiotic prescribing, identifying at-risk populations, using high-level technology, and optimizing processes to triage or refer patients to in-person care sites when needed. Together, these strategies can increase access to high-quality care and provide more robust information to guide providers when making prescribing decisions. Looking to the future, Ray also highlighted broader opportunities to use telehealth to advance antimicrobial stewardship, including enhancing access to high-quality care, providing at-distance tele-stewardship, using artificial intelligence (AI) to aid tele-diagnosis, providing video-directly observed therapy (vDOT) to support adherence, and using telehealth visits to support allergy delabeling.
Robin Patel, professor of medicine and microbiology at the Mayo Clinic, shared the importance of diagnostics to combat AMR. Worldwide, clinical decisions rely heavily on the results of diagnostic tests, she said. Patel proposed that the classic approach to diagnostics for most providers comprises three questions: Is the patient’s clinical presentation caused by an infection? If so, what is the causative pathogen? Which treatment should be administered? However, Patel suggested that this classic paradigm is no longer appropriate and proposed an approach she calls “theranostics,” where providers first determine if the patient’s clinical presentation is caused
![]()
by an infection and then assess the causative pathogen and treatment options in a single step.
Highlighting the continuous evolution of new technologies, she noted recent advances in diagnostics from rapid detection and simultaneous resistance profiling to shotgun metagenomic sequencing and advances in point-of-care tests that can improve diagnostics for antimicrobial infections. She cited the example of how advances in home-based self-testing, largely driven by the need for rapid COVID-19 antigen testing, can help develop other affordable home-based tests that enable broader access for different communities and complement telemedicine practice.
Patel envisioned that in the future, an integrated multiomics analysis could be used to test and treat antimicrobial infections. These analyses could use both microbial tests, such as culture techniques, nucleic acid amplification, and 16S ribosomal RNA sequencing, and tests that characterize host cellular or immunologic responses to provide results including likelihood of infection, predicted cause of infection, resistance genes and mutations detected, and suggested treatment regimens. Patel also noted the need for a greater focus on equitable access as new tests come to market, considering the high cost of many novel technologies.
Ritu Banerjee, professor of pediatric infectious diseases at Vanderbilt University Medical Center, spoke about the challenges and opportunities for improving inpatient antimicrobial stewardship in the United States. Half of all hospitalized patients in the United States receive antibiotics, she said, and half of these inpatient prescriptions are inappropriate (e.g., not necessary, wrong drug, or wrong dose) (Fridkin et al., 2014). Antimicrobial stewardship programs (ASPs) were created to address this problem by promoting the use of appropriate antimicrobials in the correct dose, route, and duration of treatment while minimizing toxicity, improving patient safety, and reducing health care costs. CDC has called for all hospitals to implement ASPs and defined seven core elements: leadership support, accountability, pharmacy expertise, action, tracking, reporting, and education. There has been a high degree of implementation of ASPs in hospitals across the United States, leading to the effective reduction of overall antibiotic use, increased compliance with local antibiotic policies, and decreased durations of antibiotic therapy.
Gaps remain owing to challenges in measuring factors such as clinical outcomes, appropriateness of treatment, and cost-effectiveness, she said. More resources and personnel may improve ASPs, particularly in areas such as discharge stewardship, perioperative antibiotic use, allergy delabeling, and community hospitals. Banerjee suggested moving beyond measuring simple metrics such as the number of days of treatment, and instead dedicating more resources to collecting data on outcomes that more closely reflect clinical impact such as length of hospital stay, mortality rates, resistance rates, adverse events, averted costs, and averted microbiome disruption. She also reiterated that diagnostic stewardship involves the use of the right test on the right patient at the right time, which directly relates to antimicrobial stewardship. Banerjee concluded by advocating for strategies to improve stewardship through policies that incentivize the expansion of ASPs, creating benchmarks that are adjusted for medical complexity and diagnosis, using new technologies to generate personalized risk predictions, and improving the use of outcome measures that integrate efficacy, safety, and antibiotic use.
ACCESS TO APPROPRIATE ANTIMICROBIALS
Anthony McDonnell, senior policy analyst at the Center for Global Development, noted that the majority of global AMR burden is carried by LMICs and, at the same time, lack of access to antibiotics is the main driver for AMR-associated deaths in these settings. McDonnell explained that antimicrobial procurement shortages are caused by factors such as limited market competition, institutional inefficiencies such as cumbersome registration processes and inefficient local purchasing, poor information about product quality, and high transaction costs that are passed down to purchasers. The demand for antimicrobials also fluctuates, said McDonnell, and poorer countries suffer most during a market crisis. Lack of access not only causes unnecessary deaths but exacerbates opportunities for pathogens to develop resistance.
To close the antimicrobial access gap experienced by LMICs, McDonnell advocated for the use of sustainable access hubs. Sustainable access hubs operate between manufacturers and patients, he said, creating a form of
![]()
pool procurement that facilitates reliable access to antimicrobials and diagnostics. In addition to bridging the antimicrobial access gap, sustainable access hubs reduce the inappropriate use of antimicrobials by providing diagnostics and financial and technical assistance. They also help LMICs track and report consumption data to WHO’s GLASS platform, reduce antimicrobial shortages, and reduce prices.
Jennifer Cohn, director of global access at the Global Antibiotic Research & Development Partnership (GARDP), also discussed strategies for improving antibiotic access in LMICs. She outlined barriers to access, including lack of interest from suppliers to commercialize antibiotics, lack of registration of new antibiotics in LMICs, high prices, and lack of appropriate and timely diagnostic measures to support the use of—and demand for—antibiotics. She also explained how supply-and-demand barriers are a multifaceted problem that lead to a weak distribution pipeline affecting access, availability, and affordability. Cohn shared lessons learned from the use of bedaquiline for multidrug resistant tuberculosis, where clear guidelines for use, external funding, multipartner logistical support, clinical review committees, and access to bedaquiline via importation waivers while it was awaiting registration facilitated access and use of the new antibiotic in LMICs (Guglielmetti et al., 2017).
Cohn also outlined how GARDP’s first-of-its-kind licensing agreement with Shionogi allowed for the increased access of cefiderocol, a reserve antibiotic used for serious infections, in 135 countries. Through partnership with a licensed manufacturer, registration support for commercialization, development of robust implementation plans, and evidence-based guidelines for appropriate use, Cohn explained, this case study has paved the way for stewardship-driven access of antimicrobials to LMICs. Cohn also noted that creating country-specific targets for antibiotic availability could be useful in prioritizing the supply of specific antibiotics when multiple options are available. She emphasized the need for a nuanced view in determining when to hold antibiotics in reserve and when to adopt a first-line approach.
Esmita Charani, associate professor at the University of Cape Town, discussed the challenges of creating sustainable access to antimicrobials. She reiterated that millions of deaths are caused by untreated nonresistant infections where patients lacked access to appropriate treatment. One example of the fragile and fractured supply chain system was the shortage of cefazolin in Japan, caused by a shortage of raw materials and manufacturing problems in China and Italy. This was further exacerbated by the fact that pharmaceutical organizations are not legally obligated to inform purchasers of shortages, so the purchaser was unable to prepare for the imminent supply issue.
Other reported causes for antimicrobial shortages include dwindling manufacturer interest attributable to strict regulatory requirements, price competition for off-patent agents, and inefficient procurement systems that hinder forecasting, she said. Antimicrobial shortages can have long-term consequences in both HICs and LMICs, she said. For example, the piperacillin-tazobactam shortages resulted in increased Clostridium difficile cases in the United States (Gross et al., 2017), and in Brazil, a penicillin shortage led to increased rates of congenital syphilis and stillbirths (Araujo et al., 2020). Antimicrobial shortages are also associated with increased out-of-pocket costs for patients, particularly in countries without universal health coverage, as well as increased medication errors.
More action is needed to create sustainable access, said Charani, including better communication during shortages that does not result in behaviors such as inappropriate prescribing or stockpiling. Strong legislation and political engagement requiring pharmaceutical companies to notify countries about shortages could also help alleviate some of the burden. Finally, health care systems need to be robust enough to monitor and forecast for shortages and changes in demand, she concluded.
INNOVATION IN ANTIBIOTIC DEVELOPMENT
The number of new resistant bacterial strains has been growing over the decades, said James Collins, Termeer Professor of Medical Engineering & Science and professor of biological engineering at the Massachusetts Institute of Technology, but fewer antibiotics have been developed. He discussed the application of AI, specifically machine learning (ML) and deep learning, to accelerate antibiotic discovery. Collins and his team initially used ML to reverse engineer natural molecular networks in bacterial cells to gain insights on the bactericidal mechanisms of
![]()
antibiotics and how resistance mechanisms develop. They discovered that antibiotics trigger stress responses and related compensatory mechanisms in bacteria, resulting in energetically demanding processes that ultimately lead to DNA damage. These findings led to the idea of inhibiting DNA damage response or targeting energy production to boost the effectiveness of existing antibiotics. Applying deep learning methods to analyze thousands of compounds, Collins’s team identified the compound halicin as a potent antibiotic that acted via a novel antibacterial mechanism (Stokes, 2020). They also found that halicin is effective against MDROs and has a favorable resistance profile across a panel of bacterial species.
Collins commented that deep learning models can be a “black box” that provides an output without insight into the processes guiding the decision, so his team has been working to open up the trained deep learning models to make them more transparent and interpretable. They have also advanced from discovering new antibiotics to designing them using generative AI approaches. While he believes the field offers much promise, there are still significant gaps in the ability to synthesize molecules designed by generative AI models.
Ken Duncan, deputy director of drug discovery at the Bill & Melinda Gates Foundation, discussed the TB Drug Accelerator, a public–private partnership (PPP) that has worked to accelerate drug discovery for new antibiotics against tuberculosis (TB) since 2012 (Aldridge, 2021). Highlighting the global burden of TB, he noted that more than 10 million people fall ill each year with the disease, resulting in 1.3 million deaths, including cases of drug-resistant TB (WHO, 2023). The TB Drug Accelerator aims to develop a pan-TB regimen that can treat any TB infection without the need for susceptibility testing. To achieve this challenging goal, the PPP brings together pharmaceutical companies, biotechnology and nonprofit research institutes, and academic researchers to share their data, expertise, and resources. Their approach involves phenotypic screening of compound libraries, identifying potential targets, and further analyzing potential targets through models. This accelerator has resulted in 12 clinical drug candidates, he added, with seven still actively undergoing trials.
Duncan reviewed several key features of the TB Drug Accelerator model: focusing on a specific problem, bringing together diverse stakeholders with different skills, establishing a consortium and data-sharing agreement, having a portfolio management team that includes a scientific advisory panel, and having overarching project leadership from the Gates Foundation. He emphasized the cost-effectiveness of a consortium–PPP model that also allows for innovation and reduces redundancy. Given the breadth of the AMR field, he saw potential for the application of this approach but cautioned about the need to focus on narrow indications to keep the program manageable.
Ramy Elshaboury, director of clinical pharmacy services at Massachusetts General Hospital, shared his perspective as an infectious disease pharmacist and antimicrobial stewardship clinician on the challenges of applying innovative treatments in clinical practice. He highlighted that traditional market mechanics and current reimbursement models are failing to support innovation and best practices in the clinical application of new antibiotics. Infectious disease treatment courses are typically defined with a start and end, he said, unlike other disease states where treatments can be lifelong. As a best practice for antimicrobial stewardship, novel treatments should be protected and not overused to maintain their effectiveness. However, this leads to fewer doses used and less volume sold, hindering the uptake of innovative treatments.
There have been some successful efforts on “push” incentives, he said, supporting early research and development and expediting regulatory review, but less so on “pull” mechanisms, supporting early market entry in a way that is decoupled from fee-per-unit models that put pressure on the market to increase the unit price given the limited use. For example, the New Technology Add-on Payment (NTAP) is a pull incentive in the United States. Though NTAP provides additional reimbursement beyond the diagnosis-related group (DRG) bundle payment for innovative treatments, it is limited in scope and duration, and is administratively complex, he noted. It also incentivizes a higher volume of doses, which is at odds with antimicrobial stewardship practices.
![]()
Elshaboury stated that an ideal pull incentive model would decouple reimbursement from the bundled DRG, with guaranteed reward at market entry for innovative treatments and be sustainable for several years. It would also apply to all patients, not just those using Medicare/ Medicaid, encourage clinical application and antimicrobial stewardship best practices, and be underpinned by accountability, he said. In conclusion, Elshaboury emphasized the urgent need for new payment models to support pull incentives, the customized solutions needed given the uniqueness of the antimicrobial resistance field, and the importance of PPPs in driving successful initiatives in the field.
REFERENCES
Aldridge, B. B., D. Barros-Aguirre, C. E. Barry III, R. H. Bates, S. J. Berthel, H. I. Boshoff, K. Chibale, X-J. Chu, C. B. Cooper, V. Dartois, K. Duncan, N. Fotouhi, F. Gusovsky, P. A. Hipskind, D. J. Kempf, J. Lelièvre, A. J. Lenaerts, C. W. McNamara, V. Mizrahi, C. Nathan, D. B. Olsen, T. Parish, H. M. Petrassi, A. Pym, K. Y. Rhee, G. T. Robertson, J. M. Rock, E. J. Rubin, B. Russell, D. G. Russell, J. C. Sacchettini, D. Schnappinger, M. Schrimpf, A. M. Upton, P. Warner, P. G. Wyatt, and Y. Yuan. 2021. The Tuberculosis Drug Accelerator at year 10: What have we learned? Nature Medicine 27:1333-1337.
American College of Surgeons. 2022. National Surgical Quality Improvement Program-Pediatric Surgical Antimicrobial Prophylaxis Semiannual Report. Chicago, IL: American College of Surgeons.
Antimicrobial Resistance Collaborators. 2022. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 399(10325):P629-P655. https://doi.org/10.1016/S0140-6736(21)02724-0.
Araujo, R., A. Souza, and J. Braga. 2020. Who was affected by the shortage of penicillin for syphilis in Rio de Janeiro, 2013-2017. Revista de Saude Publica (54):109.
Berglund, F., S. Ebmeyer, E. Kristiansson, and D. G. J. Larsson. 2023. Evidence for wastewaters as environments where mobile antibiotic resistance genes emerge. Communications Biology 6(1):321.
Freifeld, A. G., E. J. Bow, K. A. Sepkowitz, M. J. Boeckh, J. I. Ito, C. A. Mullen, I. I. Raad, K. V. Rolston, J.-A. H. Young, and J. R. Wingard. 2011. Executive summary: Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clinical Infectious Diseases 52(4):427-431.
Fridkin, S., J. Baggs, R. Fagan, S. Magill, L. A. Pollack, P. Malpiedi, R. Slayton, K. Khader, M. A. Rubin, M. Jones, M. H. Samore, G. Dumyati, E. DoddsAshley, J. Meek, K. Yousey-Hindes, J. Jernigan, N. Shehab, R. Herrera, C. L. McDonald, A. Schneider, A. Srinivasan, and the Centers for Disease Control and Prevention. 2014. Vital signs: Improving antibiotic use among hospitalized patients. Morbidity Mortality Weekly Report 63(9):194-200.
Gafter-Gvili, A., A. Fraser, M. Paul, L. Vidal, T. A. Lawrie, M. D. van de Wetering, L. C. Kremer, and L. Leibovici. 2012. Antibiotic prophylaxis for bacterial infections in afebrile neutropenic patients following chemotherapy. Cochrane Database Systematic Review 1(1):CD004386.
Gross, A. E., R. S. Johannes, V. Gupta, Y. P. Tabak, A. Srinivasan, and S. C. Bleasdale. 2017. The effect of a piperacillin/tazobactam shortage on antimicrobial prescribing and Clostridium difficile risk in 88 US medical centers. Clinical Infectious Diseases 65(4):613-618.
Guglielmetti, L., C. Hewison, Z. Avaliani, J. Hughes, N. Kiria, N. Lomtadze, N. Ndjeka, S. Setkina, A. Shabangu, W. Sikhondze, A. Skrahina, N. Veziris, and J. Furin. 2017. Examples of bedaquiline introduction for the management of multidrug-resistant tuberculosis in five countries. International Journal of Tuberculosis and Lung Disease 21(2):167-174.
He, K., R. B. Nayak, A. C. Allori, B. K. Brighton, R. A. Cina, J. S. Ellison, M. J. Goretsky, K. R. Jatana, M. R. Proctor, C. Grant, V. M. Thompson, M. Iwaniuk, M. E. Cohen, J. M. Saito, B. L. Hall, J. G. Newland, C. Y. Ko, and S. J. Rangel. 2022. Correlation between postoperative antimicrobial prophylaxis use and surgical site infection in children undergoing nonemergent surgery. JAMA Surgery 157(12):1142-1151.
![]()
Larsson, D. G. J., and C.-F. Flach. 2022. Antibiotic resistance in the environment. Nature Reviews Microbiology 20(5):257-269.
McKinnell, J. A., R. D. Singh, L. G. Miller, K. Kleinman, G. Gussin, J. He, R. Saavedra, T. D. Dutciuc, M. Estevez, J. Chang, L. Heim, S. Yamaguchi, H. Custodio, S. K. Gohil, S. Park, S. Tam, P. A. Robinson, T. Tjoa, J. Nguyen, K. D. Evans, C. E. Bittencourt, B. Y. Lee, L. E. Mueller, S. M. Bartsch, J. A. Jernigan, R. B. Slayton, N. D. Stone, M. Zahn, V. Mor, K. McConeghy, R. R. Baier, L. Janssen, K. O’Donnell, R. A. Weinstein, M. K. Hayden, M. H. Coady, M. Bhattarai, E. M. Peterson, and S. S. Huang. 2019. The SHIELD Orange County project: Multidrugresistant organism prevalence in 21 nursing homes and long-term acute care facilities in Southern California. Clinical Infectious Diseases 69(9):1566-1573.
Messacar, K., S. K. Parker, J. K. Todd, and S. R. Dominguez. 2017. Implementation of rapid molecular infectious disease diagnostics: The role of diagnostic and antimicrobial stewardship. Journal of Clinical Microbiology 55(3):715-723.
Miller, L. G., J. A. McKinnell, R. D. Singh, G. M. Gussin, K. Kleinman, R. Saavedra, J. Mendez, T. D. Catuna, J. Felix, J. Chang, L. Heim, R. Franco, T. Tjoa, N. D. Stone, K. Steinberg, N. Beecham, J. Montgomery, D. Walters, S. Park, S. Tam, S. K. Gohil, P. A. Robinson, M. Estevez, B. Lewis, J. A. Shimabukuro, G. Tchakalian, A. Miner, C. Torres, K. D. Evans, C. E. Bittencourt, J. He, E. Lee, C. Nedelcu, J. Lu, S. Agrawal, S. G. Sturdevant, E. Peterson, and S. S. Huang. 2023. Decolonization in nursing homes to prevent infection and hospitalization. New England Journal of Medicine 389(19):1766-1777.
Nanayakkara, A. K., H. W. Boucher, V. G. Fowler Jr., A. Jezek, K. Outterson, and D. E. Greenberg. 2021. Antibiotic resistance in the patient with cancer: Escalating challenges and paths forward. CA: A Cancer Journal for Clinicians 71(6):488-504.
Stokes J. M., K. Yang, K. Swanson, W. Jin, A. CubillosRuiz, N. M. Donghia, C. R. MacNair, S. French, L. A. Carfrae, Z. Bloom-Ackermann, V. M. Tran, A. Chiappino-Pepe, A. H. Badran, I. W. Andrews, E. J. Chory, G. M. Church, E. D. Brown, T. S. Jaakkola, R. Barzilay, and J. J. Collins. 2020. A deep learning approach to antibiotic discovery. Cell 180(4):688-702.e13.
Teillant, A., S. Gandra, D. Barter, D. J. Morgan, and R. Laxminarayan. 2015. Potential burden of antibiotic resistance on surgery and cancer chemotherapy antibiotic prophylaxis in the USA: A literature review and modelling study. Lancet Infectious Disease 15(12):1429-1437.
WHO (World Health Organization). 2023. Tuberculosis. https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed August 21, 2024).
Zheng, Y., Y. Chen, K. Yu, Y. Yang, X. Wang, X. Yang, J. Qian, Z. X. Liu, and B. Wu. 2021. Fatal infections among cancer patients: A population-based study in the United States. Infectious Diseases and Therapy 10(2):871-895.
![]()
DISCLAIMER This Proceedings of a Workshop—in Brief has been prepared by Megan Snair as a factual summary of what occurred at the meeting. The statements made are those of the rapporteur or individual workshop participants and do not necessarily represent the views of all workshop participants; the planning committee; or the National Academies of Sciences, Engineering, and Medicine.
The National Academies of Sciences, Engineering, and Medicine’s planning committees are solely responsible for organizing the workshop, identifying topics, and choosing speakers. The responsibility for the published Proceedings of a Workshop—in Brief rests with the institution.
MEMBERS OF THE WORKSHOP PLANNING COMMITTEE Jomana Musmar (Chair), Presidential Advisory Council on Combating Antibiotic Resistant Bacteria; Christopher Braden, U.S. Centers for Disease Control and Prevention; Gregory Frank, Merck & Co., Inc.; Elizabeth D. Hermsen, Pfizer, Inc.; Ramanan Laxminarayan, One Health Trust; Robin Patel, Mayo Clinic; Julia Szymczak, University of Utah School of Medicine; Matthew Zahn, Orange County Health Care Agency.
REVIEWERS To ensure that it meets institutional standards for quality and objectivity, this Proceedings of a Workshop—in Brief was reviewed by John Rex, F2G Ltd., and Casey Sullivan, U.S. Department of Health and Human Services. Leslie Sim, National Academies of Sciences, Engineering, and Medicine served as the review coordinator.
SPONSORS This workshop was partially supported by American Society of Tropical Medicine and Hygiene; Burroughs Wellcome Fund; Centers for Disease Control and Prevention; Department of Veterans Affairs; EcoHealth Alliance; Infectious Diseases Society of America; Johnson & Johnson; Merck & Co., Inc.; National Institute of Allergy and Infectious Diseases, National Institutes of Health; New Venture Fund; Rockefeller Foundation; Sanofi Vaccines; Society of Infectious Diseases Pharmacists; Uniformed Services University of the Health Services; and U.S. Agency for International Development.
STAFF Julie Liao, Forum Director; Elizabeth Ashby Guo, Program Officer; Claire Biffl, Research Associate; Taylor Windmiller, Senior Program Assistant.
For additional information regarding the workshop, visit https://www.nationalacademies.org/our-work/assessing-the-burden-of-antimicrobial-resistance-a-workshop-on-potential-policy-options-to-support-scientific-innovation.
SUGGESTED CITATION National Academies of Sciences, Engineering, and Medicine. 2024. Assessing the burden of and potential strategies to address antimicrobial resistance: Proceedings of a workshop—in brief. Washington, DC: National Academies Press. https://doi.org/10.17226/28039.












